JOINTS 2023;
1: e499
DOI: 10.26355/joints_20234_499
Deficit in hip external rotation and lumbar mobility adaptations during “turnout” performing is linked to low back pain in young pre-professional ballet dancers
Topic: Hip
Category: Original article
Abstract
OBJECTIVE: The turnout is the extreme external rotation of the lower limbs, so as to form a perfect 180° angle with the feet. It is well known that the lordosis and lumbar rotation increase in classical dance are often a form of compensation for a limited turnout due to insufficient external rotation hip range of motion. There is strong evidence that these compensatory movements predispose to the development of low back pain in dancers.SUBJECTS AND METHODS: 59 dancers (32 with no low back pain and 27 with low back pain) were involved in our study. Low back pain severity was quantified with a Numerical Rating Scale. The movements of the pelvis during the turnout were measured with an inertial sensor IMU (BJY61) positioned on S1-S2, while the passive hip external rotation was measured with a universal goniometer.
RESULTS: Measurement of the mean hip passive external rotation is respectively 45°±8° in dancers with low back pain, while dancers without low back pain measured 51°±7° with a p-value < 0.01. Analysis of the pelvic movement in the sagittal plane showed that dancers with low back pain had an increase in anterior tilt (mean 5.34°±1.89°), while dancers without low back pain had lower degrees of anterior tilt (mean 3.19°±1.45°). This difference was significant (p-value < 0.01). In addition, the linear regression showed that the increase of pelvic anterior tilt angles, during the turnout in dancers with LBP, was related to the decrease of the hip ROM in external rotation (Pearson’s coefficient r = -0.64). The odds ratio of developing low back pain was 7.5 (CI 95%: 1.50-37.45).
CONCLUSIONS: Ballet dancers have a greater risk of low back pain if they reach a turnout position that is greater than their available bilateral passive hip external rotation range of motion.
Introduction
Several studies state1-3 that there is a correlation between hip mobility and low back pain (LBP); although not confirmed, there is evidence2,3 that a reduction in the hip mobility increases lumbopelvic kinematics. Many authors1-3 have studied the relationship between LBP and decreased range of motion (ROM) in hip rotation of athletes that require extreme hip rotation, full ROM and trunk mobility. In particular, tennis players4 and professional golfers5 have been studied and very few studies1-3 focused on dancers; therefore, this study investigated the specific example of ballet dancers. It is already well known6-8 that the simultaneous in hip and trunk mobility in ballet forces the spine to assume “end range” positions (i.e., the extremes of joint capabilities) and extreme compressive and rotational forces. Although LBP is known to be a multi-factorial disease, certain studies1,2,4 suggested that a deficit in hip rotation ROM may cause LBP in athletes. Several authors9-11 have shown that the increase in spine lordosis and lumbar rotation are often compensations adopted as a consequence of an incorrect turnout performance technique. Turnout is one of the basic dance positions and it consists in the external rotation (ER) of the lower limbs, which should correspond to 180°, respectively made of hip ER of 70°, tibial ER of 5° and ankle eversion of 15°11,12 (Figure 1).
Figure 1. The turnout position.

From previous literature, we can deduce that hip ER can be limited by different factors like tightness of ileofemural and/or pubofemoral ligaments, muscular or capsular stiffness13, and structural alterations of the femur or the acetabulum (i.e., femoroacetabular impingement – FAI)14,15. Notably16, there are three morphologies of FAI: cam, pincer, and mixed. A cam-type morphology has an aspherical femoral head due to adventitious bone formation along the head-neck junction of the femur. This morphology results in impingement of the superior acetabulum with hip flexion and internal rotation. A pincer-type morphology, commonly associated with acetabular retroversion, results from the overcoverage of the femoral head. A mixed-type morphology has both cam and pincer morphologies, which is more common than in isolation16.
One additional condition that leads to a decrease in the hip ER limitation is the femur and acetabular anteversion; increased femoral anteversion (>20°), known as excessive femoral anteversion, is associated with anterior acetabular labral tears, developmental hip dysplasia, decreased ER and increased internal rotation ROM and pincer-type FAI17-20. However, a decrease hip ER has been shown21 to be related to mechanical lumbopelvic alteration. Numerous studies22,23 have analyzed the lumbopelvic compensations adopted by dancers with limited hip ER ROM. The findings of these studies show an increase in the lumbar lordosis, an increase of the anterior tilt and pelvic rotation towards the hip with reduced ER. These alterations increase the loads on the lumbopelvic girdle and can provide collective microtrauma on muscles, ligaments, capsules and discs24,25. There is evidence26 that these microtrauma in the continuum can lead to macrotrauma.
Our study has the objective of analyzing the lumbopelvic kinematic quantifying the pelvic movement with an inertial sensor (IMU), comparing the hip ER ROM between female dancers with or without LBP27-29. Our hypothesis is that dancers with LBP could also have limited hip ER and increased compensatory lumbopelvic movements.
Subjects and Methods
Study Design
Our study is an analytical cross-sectional study and aims at analyzing the lumbopelvic kinematic, quantifying the pelvic movement with an inertial sensor (IMU), comparing the hip ER ROM between dancers with or without LBP.
Setting and Participants
All the ballet dancers of the 1st Academic Year of the Licei Coreutici of Busto Arsizio and Milan were recruited for this study. Dancers were recruited in one week, from the 12th to 18th of September 2019. Each of the dancers signed a written consent form.
The study consists of 59 dancers (27 with LBP and 32 without LBP) between 13-15 years old (13.8±0.56) and training 4 hours per day. The recruited subjects were provided all of the verbal and written information regarding the study and they all understood the objectives of the study. The inclusion criteria, in addition to age, consisted of female gender dancers with at least 5 years of ballet training.
Exclusion criteria were: male gender, structural abnormalities of the spine (Adams forward bending tested negative, scoliometre < 5°), negative anamnesis for microfracture or stress fractures at the spine and lower limbs and/or lower limb or trunk surgery. Dancers in the LBP group had to declare chronic or acute LBP symptoms in the last 12 months, while the NO LBP group would not have stated episodes of LBP in the last year. Table 1 shows sample size numerosity and characteristics.
Table 1. Subject demographics (values provided include the mean ± DS; LBP, low back pain; BMI, body mass index).
|
|
NO LBP | LBP | p-value | All dancers |
| Participants | 32 | 27 | 59 | |
| Age (years) | 13.75±0.67 | 13.92±0.38 | 0.244 | 13.83±0.56 |
| Height (cm) | 161.16±6.71 | 162.44±5.69 | 0.423 | 161.75±6.25 |
| Weight (kg) | 46.92±6.07 | 49.056±5.23 | 0.163 | 47.90±5.75 |
| BMI (kg/m2) | 17.99±1.44 | 18.58±1.71 | 0.159 | 18.27±1.57 |
| Years of training | 7.31±1.91 | 7.11±2.18 | 0.706 | 7.22±2.02 |
| Training: hours/per week | 9.93±0.91 | 9.74±0.76 | 0.389 |
9.85±0.85 |
Variables
Investigated variables were pelvic movements (anterior tilt, pelvic rotations and pelvic inclination) and angular speed movements (in anterior tilt and pelvic rotation) during turnout in dancers with and without LBP. Moreover, mean passive hip ER in dancers with and without LBP was assessed.
Data Sources/Measurement
A blind examiner regarding the project of this current study and the dancers’ belonging to the LBP group and the NO LBP, recorded measurements of weight and height of all subjects; moreover, data were collected in relation to years of training and the dance technique practiced by each dancer included in the study. Drug intake was not reported from any of the dancers involved in the study.
Passive hip ER and pelvic movements during turnout, on right and left, were measured at baseline. Moreover, chronic or acute LBP symptoms in the last 12 months with Numerical Rating Scale (NRS) for pain were reported in the same timeframe.
The Inertial Sensor (bjy-61) was equipped with three-axes-gyroscope and accelerometer (MPU6050) with a Kalman filter at high precision (available at: https://invensense.tdk.com/products/motion-tracking/6-axis/mpu-6050/) (Input tension: 3V-6V, current usage: 15 mA, volume 25.4×25.4 mm, acceleration: ±16 g, Angular speed: ±2,000°/s and output frequency 100 Hz). The sensor has been connected by Bluetooth to a laptop and angular variations have been analyzed in real time with the use of the program Mini IMU (Available at: http://www.microsoft.com/zhcn/download/details.aspx?id=17718). Data of our interest (angular movements and angular speed on three planes X, Y, Z) have been registered by a technician external to this study and with 5 years of expertise in the use of the IMU. All data were copied and recorded in Excel. For dancers included in the study, the inertial sensor was placed on S1-S2 by the same physiotherapist external to this study, by the individuation of the Supero Inferior Iliac Spines (SIPS) with an elastic band with velcrum closure (Figure 2)30.
Figure 2. Position of the IMU on S2.

Dancers performed the turnout with a planned time of 50 bpm using a metronome (Beats, Stonekick, London, UK) with the aim of time standardization of 1.2 sec request during the movement.
Reliability of the inertial sensor was measured by analyzing the pelvic kinematic of 6 dancers (3 with and 3 without LBP). After 2 minutes, the same examiner repeated the measurement and the intraclass correlation coefficient was calculated (ICC).
For the anterior tilt it resulted 0.92, for rotation it corresponded to 0.91 and for inclination 0.92. These values, as reported in various studies9, show excellent reliability.
External rotation has been detected placing the dancer in prone position with the hip in slight abduction1,31. This measurement was taken by two examiners. The first one placed the dancer in the correct position and performed the passive hip external rotation avoiding any pelvic rotation and tibial rotation. The second one measured the ROM with the articular goniometer (GIMA). The goniometer was positioned with the fulcrum on the patellar center and the fixed arm perpendicular to the ceiling, while the movable arm followed the tibial axis during rotational movement.
Pain severity was quantified by administering a NRS to the patient32.
Sample Size Calculation
The number of participants was reached thanks to the willingness to participate in the study of the two dance high schools of Milan and Busto Arsizio. No incentives for participation were provided for the schools nor for the singular participants.
Statistical Analysis
Numerous efforts were applied for minimizing the risk of bias in measuring and collecting data results: all data referring to the participant were assessed and handled by external researchers not involved with the study’s aims and procedures. Moreover, we performed confirming measurements for ascertainment of investigated data and used a reliable and valid tool for measuring. Statistical data were handled by a statistician external to the study.
We considered demographical data, pelvic movements (anterior tilt, pelvic rotation and lateral tilt), angular speed in pelvic movements (anterior tilt and pelvic rotation) and passive hip ER in LBP and in NO LBP groups as variables of interest. Low back pain severity was quantified with NRS for pain. Mean and standard deviation were calculated for all the variables: pelvic compensatory movements and their speed and hip external rotation. A two-tailed Student’s t-test was calculated to verify differences between dancers with or without LBP. Statistical meaning was defined with a p-value lower than 0.05 (α<0.05). In the regression analysis, for dancers with LBP, the Pearson’s coefficient was calculated among the pelvic compensatory movements and the hip ER and between pelvic compensatory movements and lumbar pain.
Results
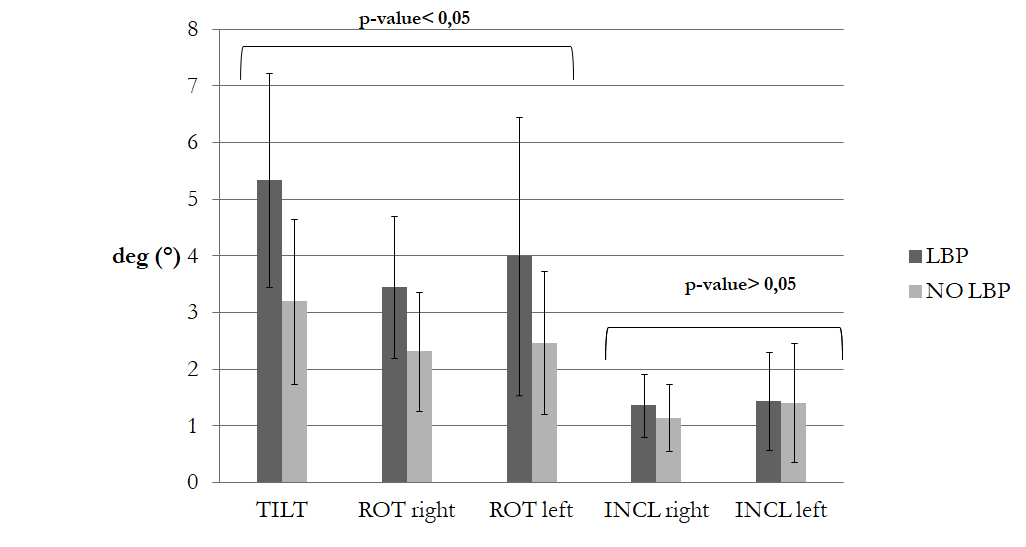
Overall, 59 female dancers were deemed to be eligible and agreed to participate in the study. Table 1 shows anthropometrics and anamnesis data with the relative p-values. The sample does not show significant differences between the variables compared at baseline (p>0.05). No missing data were reported. Measurement of the pelvic movement on the sagittal plane indicated an increase in the anterior tilt for dancers with LBP (mean 5.34°±1.89°) compared to the dancers without LBP (mean 3.19°±1.45°). This difference was statistically significant with a p-value<0.01. On the transversal plane, among the 27 dancers with LBP, 16 rotated the pelvis to the left with a rotation of 3.99°±2.45°, while the remaining 11 rotated the pelvis to the right with a rotation of 3.45°±1.25°. Among the 32 dancers without LBP, 16 rotated to the left with a rotation of 2.46°±1.26°, while the remaining 16 rotated right with a rotation of 2.32°±1.26°. Data analysis found a statistical difference between the groups with or without LBP (p-value = 0.034 for the dancers who rotated to the right and p=0.017 for the dancers who rotated to the left). On the frontal plane, there was a larger inclination of the pelvis to the right in dancers with LBP (mean 1.36°±0.55°) compared to dancers without LBP (mean 1.13°±0.59°). The pelvic inclination to the left seemed to be slightly larger in dancers with LBP (mean 1.43°±0.86°), compared to the dancers without LBP (mean 1.41°±1.05°) (Figure 3).
Figure 3. Pelvic Compensatory movement during turnout in dancers with and without LBP (TILT; anterior tilt, ROT; rotation pelvic; INCL, inclination pelvic, LBP; low back pain).
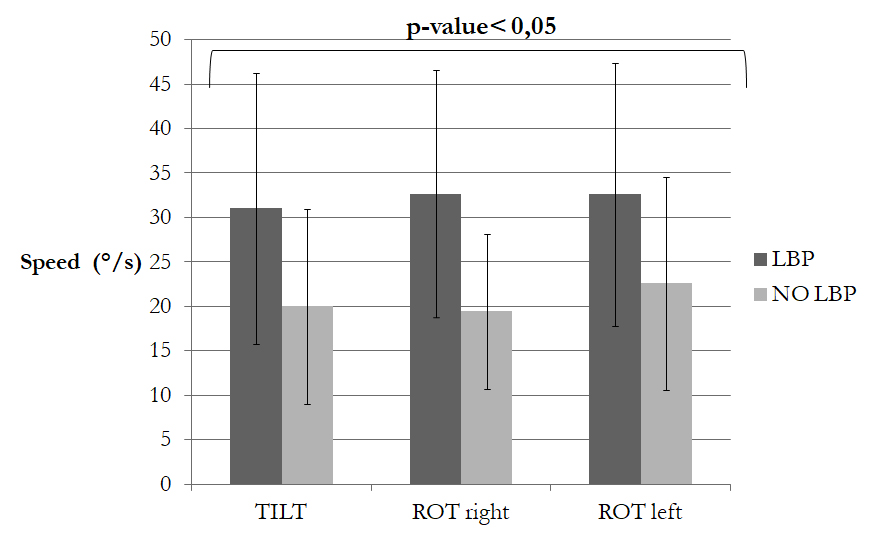
Angular speed (°/s) of the pelvic movements was significantly larger in dancers with LBP compared to dancers without LBP (p-value<0.05). The speed (°/s) of the anterior tilt for the group of dancers with LBP was 31.02°±15.23°, while it was 19.98°±10.97° for the group without LBP. Otherwise, rotation to the right for the LBP group was 32.65°±13.89°, while the rotation of no-LBP group was 19.41°±8.73°. The rotation to the left for the LBP group was 32.59°±14.81°, while the rotation of the no-LBP group was 22.59°±11.97°; in this case too, the difference in the results between the two groups was statistically significant (p-value<0.05) (Figure 4).
Figure 4. Dancers with LBP have a greater angular speed in compensatory pelvic movements than dancers without LBP (LBP; low back pain; TILT; anterior tilt, ROT; rotation pelvic).
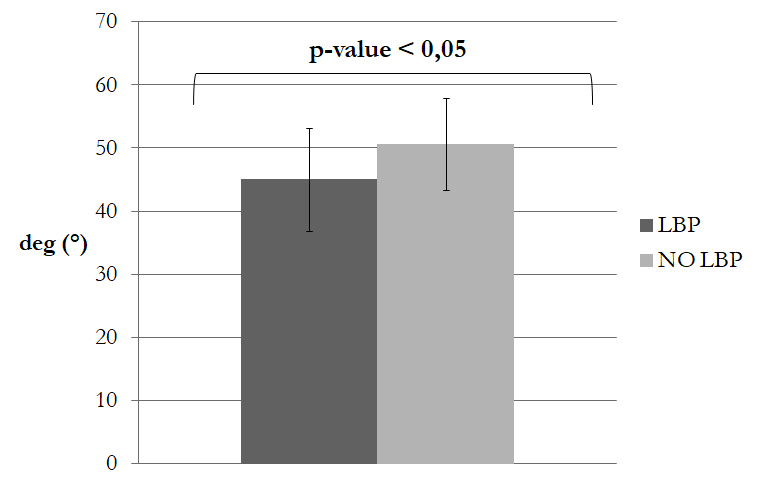
Measurement of the mean hip passive ER was 45°±8° in dancers with LBP, while in dancers without LBP was 51°±7° with a p-value <0.01 (Figure 5).
Figure 5. Dancers with LBP have a mean passive hip ER of both hips reduced than dancers without LBP.
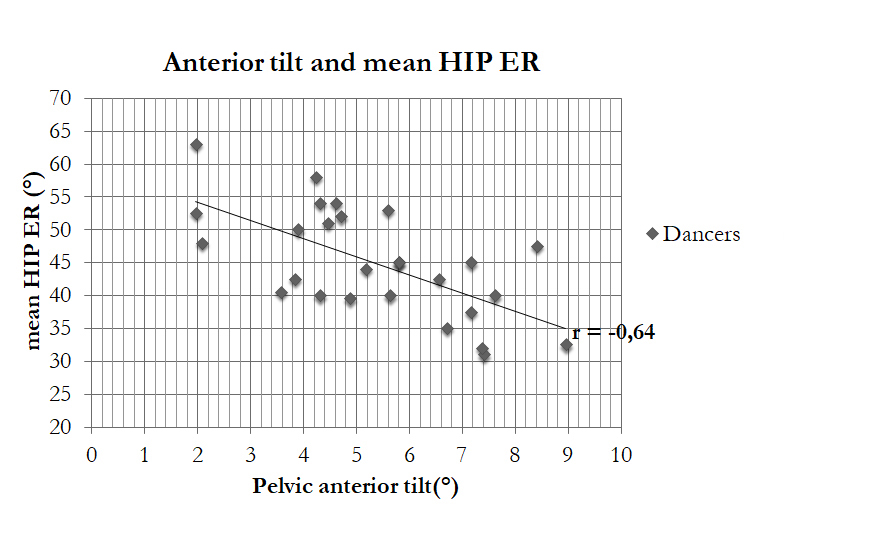
In the analysis of the data associated only to the group of dancers with LBP, the linear regression showed that the increase of pelvic anterior tilt angles was related to the decrease of the hip ROM in ER (Pearson’s coefficient r=-0.64, with a p-value<0.01) (Figure 6).
Figure 6. Correlation between anterior pelvic tilt and limitation of the hip ER in dancers with LBP.
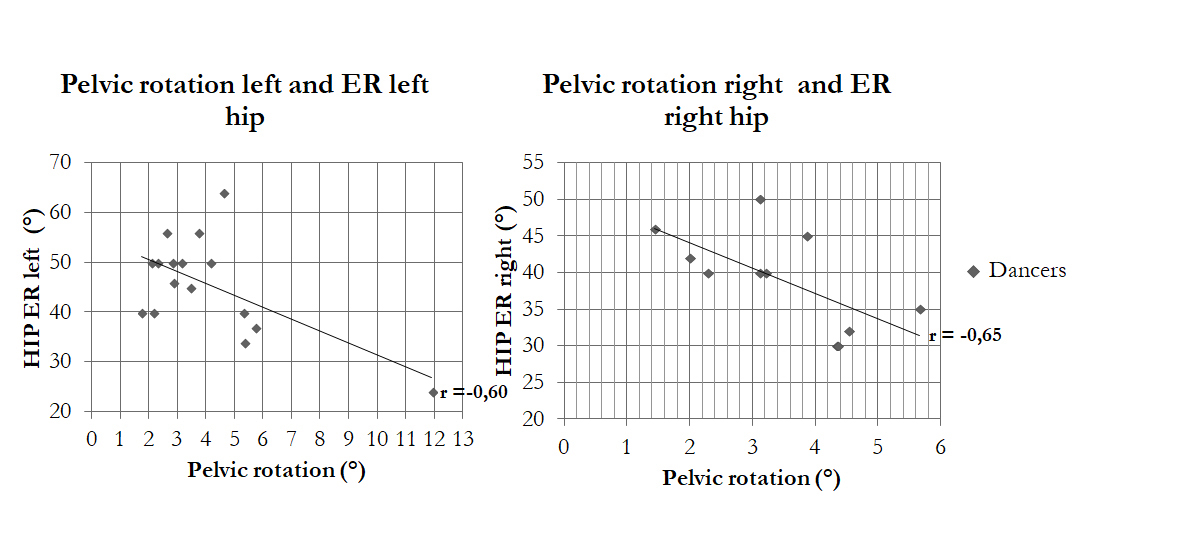
The same correlation was present in the increase of the pelvic rotation angles (for the left hip ER: r = -0.60 with p-value=0.013, while for the right hip ER: r=-0.65 with a p-value=0.031) (Figure 7).
Figure 7. Correlation between pelvic rotation and hip ER limitation in dancers with LBP.
Moreover, we observed a high correlation between the increase of the anterior tilt and the severity of LBP measured with a NRS scale (r=0.73 with a p-value<0.01) (Figure 8).
Figure 8. Correlation between pelvis anterior tilt and LBP.

There was a weak correlation between pelvic rotation and the LBP severity measured with the NRS scale (r=0.13, p-value=0.53). To calculate the odds ratio of dancers with both a pelvic rotation and anterior tilt higher than 3°, we created a tab 2X2. Dancers with LBP who perform pelvic rotation and anterior tilt greater than 3° were 25, while those without LBP were 20. Otherwise, dancers with LBP that during turnout did not perform a pelvic rotation and an anterior tilt greater than 3° were 2, while there were 12 dancers without LBP. We calculated the odds ratio between the observed frequencies ratio of 7.5 with an interval confidence of 95% (1.50-37.45).
Discussion
The first aim of this study is the measurement of the pelvic movements during turnout, comparing ROM in hip ER between dancers with or without LBP. According to findings, dancers in the recruited sample with ROM limitation in ER show greater lumbopelvic movements compared to the dancers with a greater ROM in ER. Coplan2 states that dancers with a limitation in ER and a history of LBP, in order to reach their best turnout, increase the lumbar lordosis by increasing the degrees in their anterior pelvic tilt2. This theory is in compliance with data from our study, which shows a significant increase of anterior tilt in dancers with hip limitation. A biomechanics analysis of this compensation was elaborated by Coplan2 himself, who stated that dancers who cannot reach an ideal turnout position can force turnout and increase their lumbar lordosis by anteriorly tilting the pelvis. This tilt of the pelvis allows increased ER at the hip because the acetabular shelf is much deeper posterosuperiorly than posteroinferiorly, allowing greater movements of roll and slide of the femoral head. Such data have an important clinical relevance since, as substantiated by several authors33-35, hyper-lordotic posture is one of the most important concurrent causes of LBP and can lead to spondylolisthesis. The second lumbopelvic movement analyzed is pelvic rotation. Recent studies1,2,36 state that subjects who force the spine to frequent rotations have higher risks of LBP. Moreover, we can deduct from literature37 that trunk rotation is considered as a risk factor to recurrency and chronicity of LBP. Finally, Gordon et al9 showed that lumbar rotation can generate shear stresses on the collagen fibers of the anulus and produces microscopic lesions on the spinal structure. Our results suggest that pelvic rotation in 81% of the dancers in the recruited sample happens towards the hip with reduced ROM in ER.
We can therefore formulate the following hypothesis: in the presence of a hip ROM limitation in ER, the dancer’s spine could develop a relative susceptibility in a compensatory rotation due to the gesture repetitiveness to reach the maximal range of motion of the hip and trunk in rotation. This compensatory correlation arising from this study has an important clinical implication since identifying contributing factors to LBP could promote the adoption of correct rehabilitation strategies. Regarding the pelvic lateral tilt, the results verified that the group of dancers with LBP differed with a slight increase in the inclination, but these data were not statistically significant. The analysis of the lumbopelvic movements between the LBP group compared to the group without LBP identified a strong correlation between anterior tilt and severity of the LBP, while showing a weaker correlation between rotation and severity of pain. This finding suggests that, when performing turnout, in particular in the LBP group, there was a greater anterior tilt than in the group without LBP. It is well-known38,39 that hyper-lordotic posture, requested in ballet, causes an increase in the compressive forces on the posterior structures of the spine and an increase of stress on discs, which is the concurrent cause of the development of LBP. Concerning the dancers’ angular speed to perform lumbo-pelvic movements, the results of this study suggest that anterior tilt and rotation are greater in the LBP group than in the no-LBP group. This result finds a possible explanation in the paper by Marras et al40. These authors state that the increase in the speed of the spine movement corresponds to the increase in the degree of co-activation of the trunk muscles, linked to the increase of the stress on the spine itself41,42. Thus, muscular co-activation might be considered as a factor that alters the motor control, predisposing to LBP. Clinically, indeed, a rehabilitation plan that focuses on the modification of factors, like altered movement patterns and on the recruitment of deep muscles, which provide joint stability, could be a valid strategy to the treatment of the dancer with LBP43-46. Moreover, in this study, the linear regression analysis suggests that there is a direct correlation between the pelvic anteversion and the decrease in the hip ER. This correlation is similar in the movement analysis of pelvic rotation, and it shows that an increase of this latest movement corresponds to the decrease in the hip ER ROM. In the end, in this study, the odds ratio to develop LBP is 7.5: thus, dancers during turnout compensate with pelvic rotation and anterior tilt greater than 3° have a risk 8 times higher to develop LBP. Since we hypothesize that it could be a predictive value, this represents a critical point to be discussed in regard of predisposing factors for LBP in many athletes. It is known, in fact, that LPB has a multifactor etiology47 and includes biopsychosocial factors48. This means that a part of the factors is already known to have a negative prognosis for LBP onset and maintenance, therefore we cannot forget the possible concurrent biological and mechanical causes that could be part of the LBP process, as contemplated in this study. In fact, the aim of this manuscript is to analyze the relationship between spine mobility, hip ER ROM and lumbar pain during the turnout position; this means that we did not delve into the main etiopathogenetic causes of the limitation of ER which is represented by hip dysmorphism. However, the presence of this kind of dysmorphism should be taken into account by clinicians when athletes with hip ROM reduction is assessed.
We can state that a strong correlation between lumbar mobility and hip ER and LBP was detected in our sample. Indeed, dancers with a history of acute or chronic LBP, have a reduced hip ER ROM. Evidence49-52 concerning the study of the relationship between reduced hip ROM and LBP, analysis of different type of sports with rotation requests, such as tennis, golf, judo, remains unclear. Our study, with a sample made strictly of dancers’, focused on the mobility in ER, due to the importance of one of the most fundamental movements of ballet. Other studies, as the ones collected in the review by Sadeghisani et al41, sustain the presence of the relation between patients with LBP and hip ER limitation. Overall, observing athletes who regularly practice a sport involving a rotation of hip and trunk could lead to the theory complex praxis as the sport’s mobility joint deficit tends to be compensated by the adjacent. Probably, these compensations do not seem to be always virtuous and tend towards a gesture optimization, but rather are correlated to an increase of LBP. As Sahrmann et al43 stated, the repetitive spine movement in a specific direction during specific functional and sport activities, modifies the tissue flexibility and increases the risk of LBP. Indeed, selecting patients based on activity, considering frequency, duration and intensity, should be a relevant inclusion criterion.
Based on our knowledge, this is the only study realized on dancers that analyses the relationship between spine mobility, hip ER ROM and lumbar pain during the turnout position.
Limitations
This study presents several limitations that deserve further discussion. First of all, inclusion of only female athletes could limit the generalization of results, since these cannot be transferred to a different sample of male dancers. Moreover, dancers with LBP are not classified based on different pain typology and further studies could be implemented using LBP classification system as the one suggested by the Movement Syndromes Impairment (MSI)43, which is based on the painful movement in order to classify LBP. Another limit of our study is that it analyses the pelvic movement positioning only with the IMU, avoiding the detection of strength of stabilizing muscles of the spine nor different compensatory sites, as the knee and the foot, that are widely documented in literature2,52-54. Moreover, no statistical calculation of sample size was provided. In conclusion, a further limit consists in the lack of the study of the hip and trunk muscles timing during turnout and neural factors that could be relevant in contributing to LBP55,56.
Future studies are necessary to verify if these findings could be also observed in a sample composed by dancers of different age, education and geographic origin. The measurement of pelvic movement using IMU during turnout, could be included in the dancers’ screening and we should hypothesize a research branch to assess the efficacy of an intervention focused on the identified factors and their influence on the incidence rate of LBP.
Associated measurement of strength of stabilizing muscles of the spine and ROM of different compensatory sites, as the knee and the foot, should be taken into consideration when future research on this topic is structured.
Conclusions
In the recruited sample, a correlation has been observed between LBP and an increase in the lumbo-pelvic movement of the dancers with a reduced hip ER ROM. Moreover, findings suggest that pelvic rotation and anterior tilt are factors that could be contributing to LBP in this kind of population. Our findings also suggest that clinicians should pay particular attention to assessing pelvic rotation and anterior tilt during turnout when screening dancers with LBP.
Funding
The authors have not received financial payments, support or other benefits from any commercial entity related to the subject of this article.
Conflict of Interest
The Authors declare no conflict of interest.
Informed Consent
Each of the dancers signed a written informed consent.
Ethics Approval
Not applicable.
Availability of Data and Materials
All data are available under reasonable request to the corresponding author.
ORCID ID
- Pagani: 0009-0004-4421-0875
- Baroni: 0009-0008-4022-9359
- Brindisino: 0000-0001-8950-8203
- Fasolo: 0009-0009-9063
References
- Van Dillen L, Bloom N, Gombatto S, Susco T. Hip rotation range of motion in people with and without low back pain who participate in rotation-related sports. Phys Ther Sport 2008; 9: 72-81.
- Coplan A. Ballet Dancer’s Turnout and its Relationship to Self-reported Injury. J Orthop Sports Phys Ther 2002; 32: 579-584.
- Sparkes V, Jones P. Lumbar and Pelvis Posture Changes Due to the Degree of Turnout in Ballet Dancers. World J Phys Rehab Med 2017; 1. Available at: https://www.remedypublications.com/open-access/plumbar-and-pelvis-posture-changes-due-to-the-degree-of-turnout-in-ballet-dancersp-1939.pdf.
- Vad V, Gebeh A, Dines D, Altchek D, Norris B. Hip and shoulder internal rotation range of motion deficits in professional tennis players. J Sci Med Sport 2003; 6: 71-75.
- Grimshaw P, Burden A. Case report: reduction of low back pain in a professional golfer. Med Sci Sports Exercise 2000; 32: 1667-1673.
- De Medici A, Oduoza A, Hakim B, Paton G, Retter F, Haddad A. National survey to evaluate musculoskeletal health in retired professional ballet dancers in the United Kingdom. Phys Ther Sport 2017; 23: 82-85.
- Sorensen C, Norton B, Callaghan J, Hwanga C Van Dillen L. Is lumbar lordosis related to low back pain development during prolonged standing? Man Ther 2015; 20: 553-557.
- Swain C, Bradshaw E, Whyte D, Ekegren C. The prevalence and impact of low back pain in pre-professional and professional dancers: A prospetctive study. Phys Ther Sport 2018; 30: 8-13.
- Gordon S, Yang K, Mayer P, Mace A, Kish V, Radin E. Mechanism of disk rupture – a preliminary Report. Spine (Phila Pa 1976) 1991; 16: 450-456.
- Di Cagno A, Baldari C, Battaglia C, Guidetti L, Piazza M. Anthropometric characteristics evolution in elite rhythmic gymnasts. Ital J Anat Embryol 2008; 113: 29-35.
- Hammond M. Ballet Basics. Mayfield Publishing Company 1993.
- Thomasen E. Diseases and Injuries of Ballet Dancers. Universitetsforlaget I Arhus 1982.
- Bennell K, Khan K, Matthews B. Changes in hip and ankle range of motion and hip muscle strength in 8-11 year old novice female ballet dancers and controls: a 12 month follow up study. Sports Med 2001; 35: 54-59.
- William G, Hamilton M. Tendonitis about the ankle joint in classical ballet dancers. Am J Sports Med 1977; 5: 54-88.
- Khoo-Summers L, Prather H, Hunt D, Van Dillen L. Predictors of first position turnout in collegiate dancers. Am J Phys Med Rehabil 2013; 92: 136-142.
- Griffin DR, Dickenson EJ, O’Donnell J, Agricola R, Awan T, Beck M, Clohisy JC, Dijkstra HP, Falvey E, Gimpel M, Hinman RS, Hölmich P, Kassarjian A, Martin HD, Martin R, Mather RC, Philippon MJ, Reiman MP, Takla A, Thorborg K, Walker S, Weir A, Bennell KL. The Warwick Agreement on femoroacetabular impingement syndrome (FAI syndrome): an international consensus statement. Br J Sports Med 2016; 50: 1169-1176.
- Fabry G, MacEwen GD, Shands AR Jr. Torsion of the femur. A follow-up study in normal and abnormal conditions. J Bone Joint Surg Am 1973; 55: 1726-1738.
- Beall DP, Martin HD, Mintz JQ, Costello RR, Braly BA, Yoosefian F. Anatomic and structural evaluation of the hip: a cross-sectional imaging technique combining anatomic and biomechanical evaluations. Clin Imag 2008; 32: 372-381.
- Ejnisman L, Philippon MJ, Lertwanich P, Pennock AT, Herzog MM, Briggs KK, Ho CP. Relationship between femoral anteversion and findings in hips with femoroacetabular impingement. Orthopedics 2013; 36: e293-300.
- Chadayammuri V, Garabekyan T, Bedi A, Pascual-Garrido C, Rhodes J, O’Hara J, Mei-Dan O. Passive Hip Range of Motion Predicts Femoral Torsion and Acetabular Version. J Bone Joint Surg Am 2016; 98: 127-134.
- Coryleen B, Gilbert M, Klug KB. Relationship Between Hip ER and Turnout Angle for the Five Classical ballet positions. J Orthop Sports Phys Ther 1998; 27: 339-347.
- Ryan A, Stephens R, Robert R. The Epidemiology of Dance Injuries. Dance Medicine: A Comprehensive Guide. Chicago & Minneapolis: Pluribus & The Physician and Sports Medicine 1987; 3-15.
- Solomon R. The young dancer. Clin Sports Med 2000; 19: 717-739.
- Adams M, Bogduk N, Burton K, Dolan P. 1 st ed. Edinburgh, Scotland: The biomechanics of back pain, 2002.
- McGill S. The biomechanics of low back injury: implications on current practice in industry and the clinic. J Biomech 1997; 30: 465-475.
- Jenkins J, Wyon M, Nevill A. Can turnout measurements be used to predict physiotherapist-reported injury rates in dancers?. Med Probl Perform Art 2013; 28: 230-235.
- Cuesta-Vargas A, Galán-Mercant A, Williams J. The use of inertial sensors system for human motion analysis. Phys Ther Rev 2010; 15: 462-473.
- Bolink SA, Naisas H, Senden R, Essers H, Heyligers IC, Meijer K, Grimm B. Validity of an inertial measurement unit to assess pelvic orientation angles during gait, sit-stand transfers and step-up transfers: Comparison with an optoelectronic motion capture system. Med Eng Phys 2016; 38: 225-231.
- Woo-Suck Y, Hyuno K, Hoon A. Individual characteristics of reliable lumbar coupling motions. Eur Spine J 2015; 24: 1917-1925.
- Chakraverty R, Pynsent P, Isaacs K. Which spinal levels are identified by palpation of the iliac crests and the posterior superior iliac spines? J Anat 2007; 210: 232-236.
- Ellinson J, Rose S, Sahrmann S. Patterns of hip rotation range of motion: A comparison between healthy subjects and patients with low back pain. Phys Ther 1990; 70: 537-541.
- Downie WW, Leatham PA, Rhind VM, Wright V, Branco JA, Anderson JA. Studies with pain rating scales. Ann Rheum Dis 1978; 37: 378-381.
- Gottschlich L, Young C. Spine injuries in dancers. Curr Sports Med Rep 2011; 10: 40-44.
- Alderson J, Hopper L, Elliott B, Ackland T. Risk factors for lower back injury in male dancers performing ballet lifts. J Dance Med Sci 2009; 13: 83-89.
- Tallarico RA, Madom IA, Palumbo MA. Spondylolysis and spondylolisthesis in the athlete. Sports Med Arthrosc Rev 2008; 16: 32-38.
- Harris- Hayes M, Sahrmann S, Van Dillen L. Relationship Between the hip and Low Back Pain in Atletes Who Participate in Rotation-Related Sports. J Sport Rehabil 2009; 18: 60-75.
- Skovron M. Epidemiology of low back pain. Baillieres Clin Rheumatol 1992; 6: 559-573.
- Moller A, Masharawi Y. The effect of first ballet classes in the community on various postural parameters in young girls. Phys Ther Sport 2011; 12: 188-193.
- Solomon R, Solomon J, Minton S. Preventing Dance Injuries. Champaign III: Human Kinetics 2005; 85-97.
- Marras W, Lavender S, Leurgand S. The role of dynamic three-dimensional trunk motion in occupationally- related low back disorders. Spine (Phila Pa 1976) 1993; 5: 617-628.
- Sadeghisani M, Namnik N, Karimi MT, Rafiei AR, Manshadi FD, Eivazi M, Abdoli A. Evaluation of differences between two groups of low back pain patients with and without rotational demand activities based on hip and lumbopelvic movement patterns. Ortop Traumatol Rehabil 2015; 17: 51-57.
- Hodges P, Richardson C. Altered trunk muscle recruitment in people with low back pain with upper limb movement at different speeds. Arch Phys Med Rehabil 1999; 80: 1005-1012.
- Sahrmann S. Diagnosis and Treatment on Movement Impairment Syndromes. 1st ed. St Louis: Mosby 2002; 5-118.
- Mottram S, Comerford M. A new perspective on risk assessment. Phys Ther Sport 2008; 9: 40-51.
- O’Sullivan P. Diagnosis and classification of chronic low backpain disorders: maladaptive movement and motor control impairments as underlying mechanism. Man Ther 2005; 10: 242-255.
- Samartzis D, Borthakur A, Belfer I, Bow C, Lotz JC, Wang HQ, Cheung KM, Carragee E, Karppinen J. Novel diagnostic and prognostic methods for disc degeneration and low back pain. Spine J 2015; 15: 1919-1932.
- Oliveira C, Maher C, Pinto R, Lin C, Chenot J, Van Tulder M, Koes B. Clinical practice guidelines for the management of non-specific low back pain in primary care: an updated overview. Eur Spine J 2018; 27: 2791-2803.
- Cibulka M, Sinacore D, Cromer G, Delitto A. Unilateral hip rotation range of motion asymmetry in patients with sacroiliac joint regional pain. Spine 1998; 23: 1009-1015.
- Mellin G. Decreased joint and spinal mobility associated with low back pain in young adults. J Spinal Disord 1990; 3: 238-243.
- Vad V, Bhat A, Basrai, D, Gebeh A, Aspergren D, Andrews J. Low back pain in professional golfers: The role of associated hip and low back rnage-of-motion deficits. Am J Sports Med 2004; 32: 494-497.
- Leão Almeida G, De Souza V, Barbosa G, Santos M, Saccol M, Cohen M. Swimmer’s shoulder in young athelete: rehabilitation with emphasis on manual therapy and stabilization of shoulder complex. Man Ther 2011; 16: 510-515.
- Armstrong R, Relph N. Screening Tools as a Predictor of Injury in Dance: Systematic Literature Review and Meta-analysis. Sports Med Open 2018; 4: 33.
- Cejudo A, Gómez-Lozano S, Sainz de Baranda P, Vargas-Macías A, Santonja-Medina F. Sagittal Integral Morphotype of Female Classical Ballet Dancers and Predictors of Sciatica and Low Back Pain. Int J Environ Res Public Health 2021; 18: 5039.
- Yin AX, Geminiani E, Quinn B, Owen M, Kinney S, McCrystal T, Stracciolini A. The Evaluation of Strength, Flexibility, and Functional Performance in the Adolescent Ballet Dancer During Intensive Dance Training. PM R 2019; 11: 722-730.
- Parr VA, Pettitt ML, Krzyzanowicz R, Krzyzanowicz S, Pryor RR. Type of Turnout and Injury Rates in Elite Dancers: A Critically Appraised Topic. J Sport Rehabil 2022; 31: 815-818.
- Kaufmann JE, Nelissen RGHH, Exner-Grave E, Gademan MGJ. Does forced or compensated turnout lead to musculoskeletal injuries in dancers? A systematic review on the complexity of causes. J Biomech 2021; 114: 110084.
To cite this article
Deficit in hip external rotation and lumbar mobility adaptations during “turnout” performing is linked to low back pain in young pre-professional ballet dancers
JOINTS 2023;
1: e499
DOI: 10.26355/joints_20234_499
Publication History
Submission date: 28 Feb 2023
Revised on: 08 Mar 2023
Accepted on: 22 Mar 2023
Published online: 06 Apr 2023