JOINTS 2023;
1: e655
DOI: 10.26355/joints_20237_655
A small volume of simulated loose bodies is sufficient to dramatically reduce the passive elbow range of motion: a cadaveric study
Topic: Elbow
Category: Original article
Abstract
INTRODUCTION: The presence of loose bodies in the olecranon and coronoid fossae can decrease elbow range of motion (ROM), requiring surgical removal. However, no study has quantified the ROM loss corresponding to a certain volume of loose bodies. The aim of this study was to measure the reduction of elbow extension and flexion after the introduction of a progressively increasing number of simulated loose bodies in the olecranon and in the coronoid fossa.MATERIALS AND METHODS: Ten fresh-frozen specimens with no evidence of previous trauma, instability, or gross ROM deficit were included in the study. ROM in flexion and extension was measured. A mini-open high-posterolateral approach to the olecranon fossa was performed, and a progressively increasing number of 5 mm-diameter radiopaque spheres was introduced. Fluoroscopy was used to confirm intra-articular placement, and ROM was measured after each group of spheres was introduced. After the removal of the spheres from the olecranon fossa, a mini-open over-the-top approach was performed to the coronoid fossa, and the same process was repeated.
RESULTS: The initial median total range of motion was 155° (155° flexion). The introduction of a volume of 0.2 cm3 in the olecranon fossa caused a reduction of 41.79% of the total extension. This percentage increased to 48% with 0.33 cm3 and to 51.40% with 0.46 cm3. The introduction of 0.2 cm3 in the coronoid fossa caused a reduction of 63.79% of the total flexion. This percentage increased to 71.06% with 0.33 cm3 and to 73.49% with 0.46 cm3.
CONCLUSIONS: This study quantifies the relation between the reduction of elbow ROM in extension and flexion and the number and volume of loose bodies in the olecranon and coronoid fossae. This information is precious for surgeons approaching the stiff elbow and could be relevant for preoperative counseling helping surgeons and patients develop realistic expectations.
Introduction
Loose bodies in the elbow joint can develop as a consequence of degenerative primary elbow osteoarthritis, secondary post-traumatic osteoarthritis, osteochondritis dissecans (OCD) and synovial chondromatosis and may lead to pain, range of motion (ROM) reduction, joint swelling, episodes of locking and catching as well as secondary neurologic compression syndromes1-3.
The diagnostic workup includes a plain radiograph as first-level imaging, followed by magnetic resonance imaging (MRI) and computed tomography (CT) in doubtful cases or as preoperative investigation to determine the exact count and location of the loose bodies and plan surgery accordingly. MRI has been recommended4 as more reliable and accurate than other imaging studies for differential diagnosis, nevertheless areas of mineralization, which are hypointense on all routine MRI sequences, can be best detected with CT.
The presence of loose bodies in the olecranon and coronoid fossae can dramatically decrease elbow range of motion (ROM), reducing the quality of life and requiring surgical removal to restore motion and painless function.
Nevertheless, no study has yet quantified the ROM loss corresponding to a certain volume of loose bodies located in the elbow joint. The aim of this study was to measure the reduction of elbow extension after the introduction of a progressively increasing number of simulated loose bodies in the olecranon fossa and the reduction of elbow flexion after the introduction of a progressively increasing number of simulated loose bodies in the coronoid fossa.
Materials and Methods
Ten fresh-frozen specimens of upper extremities from the fingertip to the humeral head from human donors were available for this biomechanical cadaveric study. The specimens were thawed at room temperature overnight before the experiment. Before the investigation, care was taken to evaluate the specimens for visible signs of previous trauma, gross instability, or deformity. Radiographic images were taken to visualize the integrity of the bony structures and joint congruency. None of the specimens demonstrated extension contracture, flexion contracture, or gross instability. The ROM of each elbow prior to the study beginning was measured with a graduated protractor.
To simulate the presence of intra-articular loose bodies, an increasing number of standardized 5 mm-diameter (0.066 cm3) radiopaque lead spheres were introduced into the joint linked to each other with a flexible and deformable cable in a necklace fashion. This was performed to allow insertion and extraction of the radiopaque lead spheres using a minimally invasive approach, not damaging any ligamentous structure and therefore with negligible effect on the elbow ROM.
To introduce the spheres in the olecranon fossa, the specimens were placed with lateral epicondyle facing up on a dissection table, the elbow flexed 90° and the forearm in neutral position. A single surgeon with extensive experience in arthroscopic and open elbow surgery (P.A.) performed a mini-open (< 1 cm) high-posterolateral approach to the olecranon fossa on all specimens; a group of three 5 mm-diameter radiopaque spheres (0.2 cm3 volume) was then introduced in the fossa with an arthroscopic grasper. The elbow then underwent repeated cycles of flexion-extension, in order to allow the spheres to reach the position in which they produce the least effect in terms of ROM reduction.
Fluoroscopy was then used to confirm the correct intra-articular placement of the spheres (Figure 1), and ROM was measured by an external observer and not involved in the statistical evaluation of the collected data (F.L.), with a graduated protractor centered on the lateral epicondyle and positioned parallel along the midline of the humeral shaft and the ulnar crest. The same procedure was then repeated with five (0.33 cm3) and seven (0.46 cm3) spheres.
Figure 1. Fluoroscopic image confirming the correct position of three radiopaque spheres in the olecranon fossa.

After removal of the spheres from the olecranon fossa, the elbow was placed on the dissection table with the medial epicondyle facing up and in 90° of flexion, with the forearm in neutral position; the same surgeon performed a mini-open over-the-top approach to the coronoid fossa (< 1 cm) and three 5 mm-diameter radiopaque spheres were introduced in the fossa with an arthroscopic grasper.
Fluoroscopy was used to confirm the correct intra-articular placement of the spheres, and ROM was measured with a graduated protractor at each step, as previously described. The same procedure was repeated with five and seven spheres placed in the coronoid fossa. In both surgical approaches, care was taken not to damage any ligamentous structure.
To calculate and present the ROM loss in flexion and extension in a clear and intuitive way, a 90°-flexion position was considered as starting position for the measurements and ROM after the insertion of simulated loose bodies. Two variables were hence investigated: the flexion-ROM (F-ROM = measured flexion – 90°) and the extension-ROM (E-ROM = 90° – measured extension); these values were normalized (%F-ROM and %E-ROM) to the maximal arc of flexion (full flexion without simulated loose bodies – 90°) and the maximal arc of extension (90° – full extension without simulated loose bodies). Comparisons between the full ROM without simulated loose bodies and the ROM measured after the introduction of simulated loose bodies were indicated with a D (DF-ROM, DE-ROM, D%F-ROM, and D%E-ROM).
Institutional approval of the study protocol was obtained prior to the study beginning (ICLO Research Center ID10603).
Statistical Analysis
Statistical analysis was performed using GraphPad Prism v. 6.0 software (GraphPad Software Inc. La Jolla, CA, USA). A sample size of 30 measurements for each fossa achieves 83% of power to detect a difference of -0.50000 between the null hypothesis correlation of 0.00000 and the alternative hypothesis correlation of 0.50000, using a two-sided hypothesis test with a significance level of 0.05000.
The Shapiro-Wilk normality test was used to evaluate the normal distribution of the sample. Continuous variables were expressed as median and interquartile range [first quartile – third quartile] or as mean ± standard deviation, as appropriate. Statistical evaluation of the differences among the groups was performed using one-way analysis of variance (ANOVA) with post-hoc Sidak’s multiple comparisons tests. The significance level was set at a p-value lower than 0.05.
Results
Ten specimens were included in the study (females 70%; right elbows 60%; mean age at death 75.40 ±14.71 years).
Initial median full ROM was 155° [146.25 – 160]°, with median full extension of 0° [–5 – 3.75]° and median full flexion of 155° [150 – 155]°. Herewith, a mean E-ROM of 90.80° ± 8.42° and a mean F-ROM of 63.00° ± 5.87° were obtained for the native specimens.
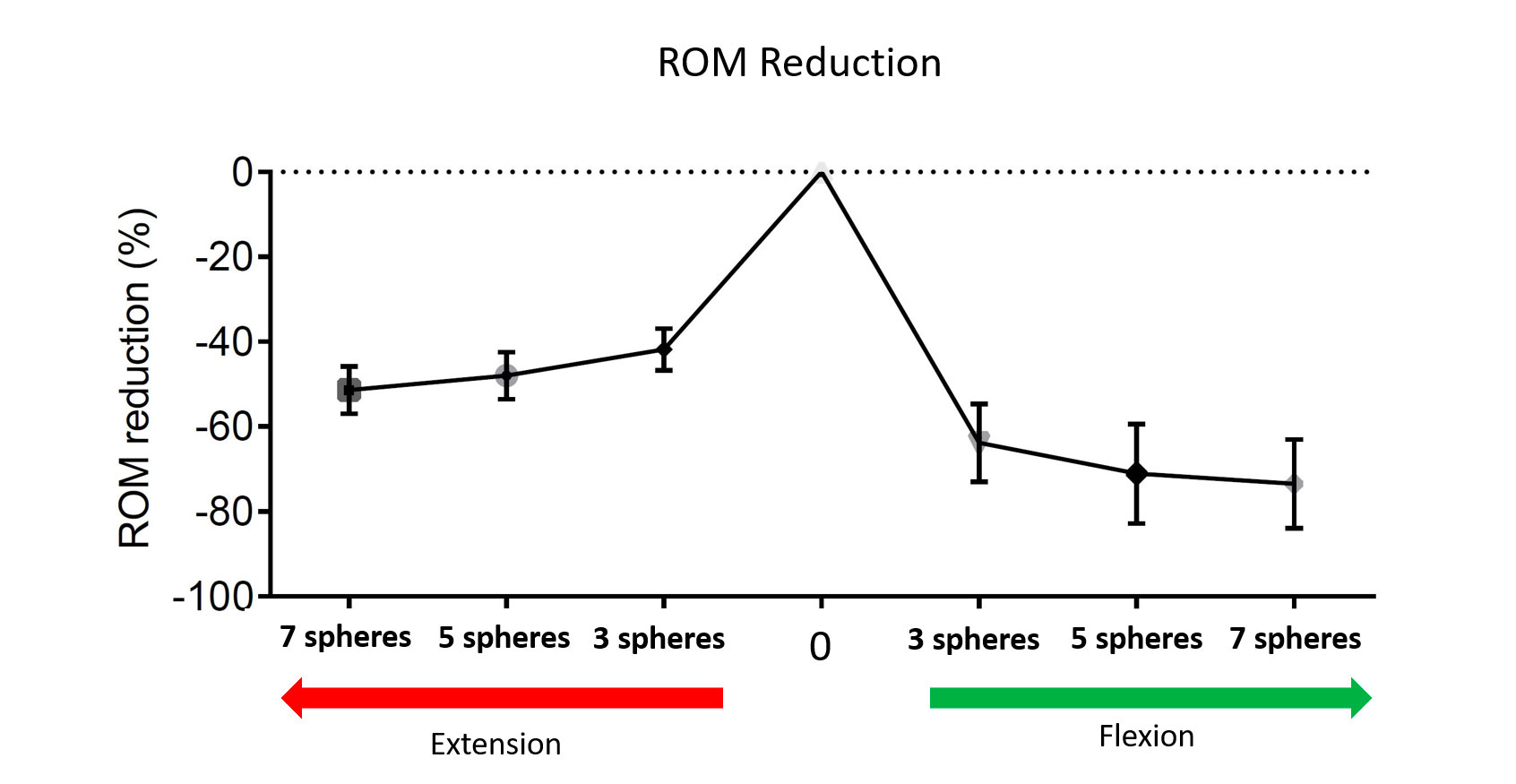
The insertion of 0.2 cm3 (three spheres) in the olecranon fossa caused a reduction of the %E-ROM of 41.79 ± 4.94% of the total extension. This percentage increased to 48 ± 5.57% with 0.33 cm3 (five spheres) and to 51.40 ± 5.58% with 0.46 cm3 (seven spheres). Significant changes were documented between each progressive step. The insertion of 0.2 cm3 (three spheres) in the coronoid fossa caused a reduction of %F-ROM of 63.79 ± 9.17% of the total flexion. This percentage increased to 71.06 ±11.69% with 0.33 cm3 (five spheres), and to 73.49 ± 10.48% with 0.46 cm3 (seven spheres). Table 1 illustrates the changes in ROM in each study condition; Figure 2 graphically summarizes the main findings of the ANOVA on the previously illustrated data.
Table 1. Percentage of ROM loss after progressive insertion of 3, 5 and 7 spheres, respectively.
| Basal condition (no spheres) (°) | Progressive filling of the olecranon fossa | 3 spheres (0.2 cm3) | 5 spheres (0.33 cm3) | 7 spheres (0.46 cm3) |
| -0.8 ± 7.98
E-ROM 90.8 ± 7.98
|
D E-ROM (°) | -38.1 ± 6.35 | -43.8 ± 7.50 | -46.8 ± 7.02 |
| D % E-ROM | -41.8 ± 4.94 | -48.0 ± 5.57 | -51.4 ± 5.58 | |
| p-value to basal condition | <0.0001 | <0.0001 | <0.0001 | |
| p-value to previous olecranon fossa filling step | <0.0150 | n.s. | ||
| Basal condition (no spheres) | Progressive filling of the coronoid fossa | 3 spheres (0.2 cm3) | 5 spheres (0.33 cm3) | 7 spheres (0.46 cm3) |
| 153.8 ± 5.57
F-ROM 63 ± 5.57 |
D F-ROM (°) | -40 ± 6.78 | -44.6 ± 7.2 | -46.1 ± 32 |
| D % F-ROM | -63.79 ± 9.17 | -71.06 ± 11.69 | -73.49 ± 10.48 | |
| p-value to basal condition | <0.0001 | <0.0001 | <0.0001 | |
| p-value to previous coronoid fossa filling step | n.s. | n.s. | ||
Continuous variables were expressed as mean ± standard deviation (SD).
Figure 2. Ordinary one-way ANOVA graph showing the 95% confidence intervals computed by Sidak’s multiple comparisons test for the percentile difference in ROM between the native ROM and the ROM obtained after inserting, respectively 3, 5 and 7 spheres in the olecranon fossa (left, reduction of Extension-ROM) and in the coronoid fossa (right, reduction of Flexion-ROM).
The differences between the groups were not statistically significant except for the comparison between loss in extension with three spheres and five spheres (Figure 3).
Figure 3. Ordinary one-way ANOVA graph showing the 95% confidence intervals computed by Sidak’s multiple comparisons test for the percentile difference in ROM loss between groups in extension and in flexion. If the confidence intervals do not include zero, this indicates that the difference between the means is statistically significant.

Discussion
The main finding of this biomechanical study is that even the presence of a small volume of simulated loose bodies can significantly reduce the total joint ROM. This study provides herewith biomechanical evidence to support procedures aimed at removing loose bodies to treat elbow stiffness, as well as a reference frame for preoperative patient counseling regarding the expected postoperative motion gain.
Loose bodies in the elbow joint can develop as a consequence of OCD, primary and secondary elbow osteoarthritis, synovial chondromatosis, or be caused by the presence of foreign bodies inside the joint capsule; loose bodies may lead to a painful or painless ROM restriction, in some cases associated with episodes of swelling, locking and catching1. Multiple or voluminous loose bodies may be responsible for secondary neurologic compression syndromes2,3.
Elbow arthroscopy has become the gold standard for the treatment of many post-traumatic and degenerative elbow diseases, with loose body removal having become one of the most common indications for arthroscopic elbow procedures4-6. Loose body removal, combined with synovectomy in cases of symptomatic synovial chondromatosis, can reduce pain, increase ROM and prevent secondary cartilage damage4-6. Clinical reports7,8 describing such procedures reported encouraging results.
Depending on the number and volumes of loose bodies, a lesser or greater restriction can occur, and the postoperative ROM gain is therefore expected to differ in each case. Unstable OCDs may create a single or few loose bodies, the removal of which can lead to an increase in ROM and improvement of pain and function, as demonstrated by Baumgarten et al9 in a clinical series of 16 adolescents (average increase in ROM after surgery of 20°) and by Micheli et al10 in a series of 47 children and adolescents (average increase in ROM after surgery of 30°, 85% good to excellent results and 90% return to sports without limitations).
On the other hand, in synovial chondromatosis, numerous loose bodies can be found inside the joint; the arthroscopic removal of these loose bodies, associated with synovectomy, is indicated in phases II and III of the disease, leading to favorable outcomes, including ROM improvement4,5,11.
Intra-articular loose bodies can also develop in osteoarthritic patients, with a prevalence reported12 by 66.6% of patients. Symptomatic osteoarthritis patients can benefit from arthroscopic loose body removal in terms of both clinical symptomatology and elbow ROM12,13.
Two critical aspects in the treatment of intraarticular loose bodies remain their diagnosis and the preoperative quantification of the expected ROM gain after removal. Clasper and Carr12 reported that radiographs had an overall accuracy of 71.7% in predicting the presence of loose bodies, confirming the need for a complete radiological study with second-level imaging; CT, CT arthrography, and MRI have been investigated as possible tools to increase the diagnostic performance, with native CT gaining popularity for the preoperative planning of elbow arthrolysis6,14-16. A potential advantage of second-level imaging is the possibility to calculate preoperatively the desired resection volume of the planned procedure, enabling an indirect quantification of ROM gain after loose bodies removal and the diagnosis of possible associated factors contributing to ROM reduction.
In this context, our study is the first to quantify ROM loss related to the presence of a defined volume at the level of the olecranon and coronoid fossae, and represents an important milestone in defining how intra-articular volumes relate to ROM loss. Specifically, our study showed a greater reduction in %F-ROM when filling the coronoid fossa. Nevertheless, the clinical relevance of this finding is also affected by the greater ROM in flexion, as compared to extension when considering a reference starting position of 90° flexion. In fact, to generate a ROM reduction in flexion greater than 50% of the maximum total flexion arc, a higher volume was necessary to generate a 50% loss of extension (0.46 cm3 vs. 0.2 cm3). These small volumes should also be interpreted considering the total volume of the elbow joint, estimated to be around 23 cm3,17.
All these findings may be of help in pre-operative clinical counseling, helping surgeons to quantify the expected ROM gain and highlighting possible alternative sources of ROM loss (for example, osteophytes and capsular contractures18), but they can also be helpful for patients to develop realistic expectations from the outcome of the surgery.
Limitations
The limitations of this study are the small number of investigated specimens, which may amplify bias related to technical aspects of the procedure and anatomical variants, and the lack of an evaluation of the interobserver reliability of the goniometric measurement. Finally, this study was not designed to investigate the safety and efficacy of specific surgical procedures on the anterior and posterior compartments of the elbow.
Conclusions
This study quantifies the relation between the volume of simulated loose bodies in the olecranon and coronoid fossae and the ROM loss in extension and flexion. Even the presence of very small volumes compared to the total volume of the elbow capsule can lead to relevant mechanical ROM impairment. This information is precious for surgeons approaching elbow stiffness and could be relevant for preoperative counseling helping patients to develop realistic expectations.
Conflict of Interest
Paolo Arrigoni declares consultancy for Arthrex, outside the submitted work. Pietro Randelli declares consultancy for Arthrex, Microport, Depuy (Johnson&Johnson) and Medacta outside the submitted work. All other authors declare no conflict of interest. All other authors have no relevant financial or non-financial interests to disclose.
Informed Consent
This article does not contain any studies with human participants performed by any of the authors, since it is a cadaveric study.
Ethics Approval
This study was performed after the ethical approval of the Nicola’s Foundation & ICLO Research Center (ID10603).
Funding
No funds, grants, or other support were received during the preparation of this manuscript.
Availability of Data and Materials
All raw and measurement data are recorded on an Excel spreadsheet and can be made available upon request to the corresponding author.
Authors’ Contributions
All authors contributed to the study conception and design. Study concept and design were elaborated by Paolo Arrigoni, Carlo Zaolino and Davide Cucchi. Material preparation and surgical set-up were performed by Paolo Arrigoni and Francesco Luceri. Data collection was performed by Ivan Picchierri and statistical analysis by Alessandra Menon. The first draft of the manuscript was written by Carlo Zaolino and Davide Cucchi and all authors commented on previous versions of the manuscript. Valentina Vismara and Pietro Randelli corrected finally the manuscript. All authors read and approved the final manuscript.
References
- Karaman I, Guney A, Doğar F, Oner M, Bilal O. Synovial chondromatosis caused mechanical snapping elbow: a case report. Open Access J Sports Med 2015; 6: 225-228.
- Yukata K, Murase M, Hashimoto T, Shimaoka Y, Taguchi T, Hamawaki J. Ulnar nerve palsy caused by synovial protrusion in synovial chondromatosis of the elbow: a case report and literature review. Shoulder Elbow 2018; 10: 128-132.
- Osma-Rueda JL, Amaya-Mujica J. Entrapment of the ulnar nerve in cubital tunnel by free intra-articular body-a case report. JSES Open Access 2017; 1: 109-112.
- Neumann JA, Garrigues GE, Brigman BE, Eward WC. Synovial Chondromatosis. JBJS Rev 2016; 4: e2.
- Flury MP, Goldhahn J, Drerup S, Simmen BR. Arthroscopic and open options for surgical treatment of chondromatosis of the elbow. Arthroscopy 2008; 24: 520-525.e1.
- Dubberley JH, Faber KJ, Patterson SD, Garvin G, Bennett J, Romano W, MacDermid JC, King GJW. The detection of loose bodies in the elbow: the value of MRI and CT arthrography. J Bone Joint Surg Br 2005; 87: 684-686.
- Griesser MJ, Harris JD, Likes RL, Jones GL. Synovial chondromatosis of the elbow causing a mechanical block to range of motion: a case report and review of the literature. Am J Orthop (Belle Mead NJ) 2011; 40: 253-256.
- Mo J, Pan J, Liu Y, Feng W, Li B, Luo K, Mo W, Lin H, Liao S. Bilateral synovial chondromatosis of the elbow in an adolescent: a case report and literature review. BMC Musculoskelet Disord 2020; 21: 377.
- Baumgarten TE, Andrews JR, Satterwhite YE. The arthroscopic classification and treatment of osteochondritis dissecans of the capitellum. Am J Sports Med 1998; 26: 520-523.
- Micheli LJ, Luke AC, Mintzer CM, Waters PM. Elbow arthroscopy in the pediatric and adolescent population. Arthroscopy 2001; 17: 694-699.
- Zhu W, Wang W, Mao X, Chen Y. Arthroscopic management of elbow synovial chondromatosis. Medicine (Baltimore) 2018; 97: e12402.
- Clasper JC, Carr AJ. Arthroscopy of the elbow for loose bodies. Ann R Coll Surg Engl 2001; 83: 34-36.
- Savoie FH 3rd, Nunley PD, Field LD. Arthroscopic management of the arthritic elbow: indications, technique, and results. J Shoulder Elbow Surg 1999; 8: 214-219.
- Zubler V, Saupe N, Jost B, Pfirrmann CWA, Hodler J, Zanetti M. Elbow stiffness: effectiveness of conventional radiography and CT to explain osseous causes. AJR Am J Roentgenol 2010; 194: W515-520.
- Kwak JM, Kim H, Sun Y, Kholinne E, Koh KH, Jeon IH. Arthroscopic osteocapsular arthroplasty for advanced-stage primary osteoarthritis of the elbow using a computed tomography-based classification. J Shoulder Elbow Surg 2020; 29: 989-995.
- Lenoir H, Carlier Y, Ferrand M, Vidil A, Desmoineaux P. Can preoperative imaging predict the outcomes after arthroscopic release for elbow arthritis? Orthop Traumatol Surg Res 2019; 105: S229-S234.
- Van Den Broek M, Van Riet R. Intra-articular capacity of the elbow joint. Clin Anat 2017; 30: 795-798.
- Steinmann SP. Elbow arthroscopy: where are we now? Arthroscopy 2007; 23: 1231-1236.
To cite this article
A small volume of simulated loose bodies is sufficient to dramatically reduce the passive elbow range of motion: a cadaveric study
JOINTS 2023;
1: e655
DOI: 10.26355/joints_20237_655
Publication History
Submission date: 05 Jun 2023
Revised on: 23 Jun 2023
Accepted on: 03 Jul 2023
Published online: 24 Jul 2023