JOINTS 2026;
4: e2013
DOI: 10.26355/joints_20265_2013
Subspine impingement: a national multicenter retrospective observational study on prevalence, diagnosis, treatment, rehabilitation, and athletic recovery
Topic: Hip
Category: Original article
Abstract
OBJECTIVE: Anterior inferior iliac spine impingement (AIIS-I) is considered a source of groin pain in players performing specific sports, often associated with femoro-acetabular impingement (FAI). Its clinical presentation is not pathognomonic, so only experienced specialists can suspect such a deformity; however, because FAI is more common and symptomatic, many AIIS-I cases are underestimated, and the actual impact of AIIS-I on symptoms and post-operative functional recovery is not yet clear. The aim of this paper is to assess the prevalence of AIIS-I in patients with groin pain syndrome managed by hip conservative surgeons over a 10-year period (2013-2023) at a national level, and to evaluate the specific treatments performed and their implications for rehabilitation and return to sport.
PATIENTS AND METHODS: A national retrospective observational study was conducted by the members of the Hip Committee of the Italian Society of Arthroscopy, Knee, Upper Limb, Sports, Cartilage, and Orthopedic Technologies (SIAGASCOT) in order to assess the prevalence of AIIS-I over a period of ten years, and their choices of treatment for patients operated for FAI.
RESULTS: The prevalence of AIIS-I was 3.19% (178 of 5,578 patients with FAI who underwent surgery). All patients presented with FAI-related symptoms; no patients with AIIS-I alone were treated. The global mean age at diagnosis was 29.45 (range: 15-56), with the majority being male patients (153 vs. 25). 150 of 178 patients (84.2%) underwent surgery for FAI and AIIS-I, while the remainder were managed for FAI alone or other lesions. No complications were recorded, and no specific rehabilitative prescriptions or modifications to return-to-sport schedules were proposed in patients with FAI + AIIS-I, compared with those with only FAI.
CONCLUSIONS: This retrospective study demonstrates that AIIS-I is an uncommon alteration, deserving attention from hip conservative surgeons and requiring surgery in cases of moderate/severe deformity or in high-level athletes affected by FAI. AIIS-I can be easily treated during arthroscopy, which is mainly performed for FAI. However, no specific rehabilitation programs or return-to-sport protocols have been reported for patients with FAI + AIIS alterations.
Introduction
Anterior inferior iliac spine impingement (AIIS-I), also known as subspine impingement (SS-I), is considered a source of groin pain in players performing specific sports, often associated with femoro-acetabular impingement (FAI). Its mechanism implies an overstress and compression between the AIIS prominence and femoral neck on the acetabular labrum and hip capsule in deep flexion or during a combination of flexion and internal rotation1-4. AIIS-I may be caused by a congenital deformity, an acquired alteration in highly active or professional sport players, or an avulsion trauma in growing athletes4. Its clinical presentation is typically unclear or pathognomonic, so only experienced specialists are able to suspect this deformity, unless standard X-rays reveal significant bone abnormalities. However, in these patients, FAI is generally the main source of symptoms; thus, many cases of AIIS-I cases are underestimated3. From a diagnostic point of view, and as mentioned, severe alterations of the AIIS shape are clearly detected at a simple X-ray evaluation: minimal or mild deformities may be underscored3,4-7. “False profile” X-ray views or computed tomography (CT) scans are useful to estimate the amount of deformity and its correlation with symptoms referred by patients1. Hetsroni et al7 first proposed a structured classification based on 3D-CT scan for the evaluation of this clinical pattern, followed by Ilizaliturri et al8, who confirmed it intra-operatively. An interesting study1 focused on the sensitivity of each diagnostic tool for AIIS-I detection, reporting values ranging from 76% to 86% for plain radiography, 80% to 81.8% for 3D-CT, 80% for magnetic resonance imaging (MRI), and 92.5% for ultrasound. The treatment may be conservative or surgical, depending on the complained symptoms and association with FAI1-4. Surgically treated or not, AIIS-I should also be considered from a rehabilitative perspective to assess potential modifications to patients’ return-to-sport protocols1. Currently, no significant differences in rehabilitation protocols arise from the literature8-11 in athletes operated on both for FAI and AIIS-I, with respect to those undergoing surgery for FAI alone. However, a few improvements in postoperative hip flexor strength and clinical scores have been observed in patients undergoing osteoplasty for FAI and AIIS-I compared with FAI alone.
Whatever the origin, AIIS-I has been considered overdiagnosed by several surgeons1, while others5,10,11 reported it as even responsible for a percentage of failures after hip arthroscopy performed for the treatment of FAI alone. However, to date, there is still debate about the impact of this bony alteration on symptoms: the prevalence appears to be about 18% in symptomatic hips in young and active patients1.
The aim of this paper is to assess the prevalence of AIIS-I in patients affected by groin pain syndrome (GPS) surgically managed by hip conservative surgeons in a period of 10 years (2013-2023) at a national level, and to evaluate the specific orthopedic treatments performed; moreover, the various diagnostic modalities, rehabilitation options, and any athletic recovery strategies were evaluated.
Patients and Methods
A national multicenter retrospective observational study, approved by the Ethical Committee of Careggi University Hospital (CEAVC_Prot. 24116 on 26/11/2024), was conducted by the members of the Hip Committee of the Italian Society of Arthroscopy, Knee, Upper Limb, Sports, Cartilage, and Orthopedic Technologies (SIAGASCOT) in order to assess the prevalence of AIIS-I over a period of ten years (2013-2023), and their choices of treatment. Inclusion criteria were all consecutive patients complaining of groin pain syndrome related to FAI, FAI + AIIS-I, or AIIS-I alone, undergoing arthroscopic or mini-open procedures; AIIS-I was evaluated using Hetsroni’s classification. Exclusion criteria were patients with incomplete medical records or no documented evaluation according to Hetsroni’s classification. Specific parameters obtained from the medical records of each center were: hospital characteristics (public, private, or mixed facilities), patients’ demographics (age, sex, affected side), main diagnosis, AIIS-I classification based on Hetsroni’s study7, imaging, type of treatment, and complications. The resulting cases were evaluated to determine the prevalence of AIIS-I among all patients managed by the committee members.
Statistical Analysis
All items were statistically analyzed using PSPP software (Free Software Foundation Inc. 2022, Boston, MA, USA) for Windows. Data obtained were entered into a comprehensive database using Microsoft Excel Package Office; the Pearson Chi-square test and Fisher’s exact test were used to study the association between the different parameters (numbers of FAI vs. FAI + AIIS-I cases, number of operated FAI vs. FAI + AIIS-I cases, and overall cases of FAI for each surgeon or center). A p-value < 0.05 was considered statistically significant.
Results
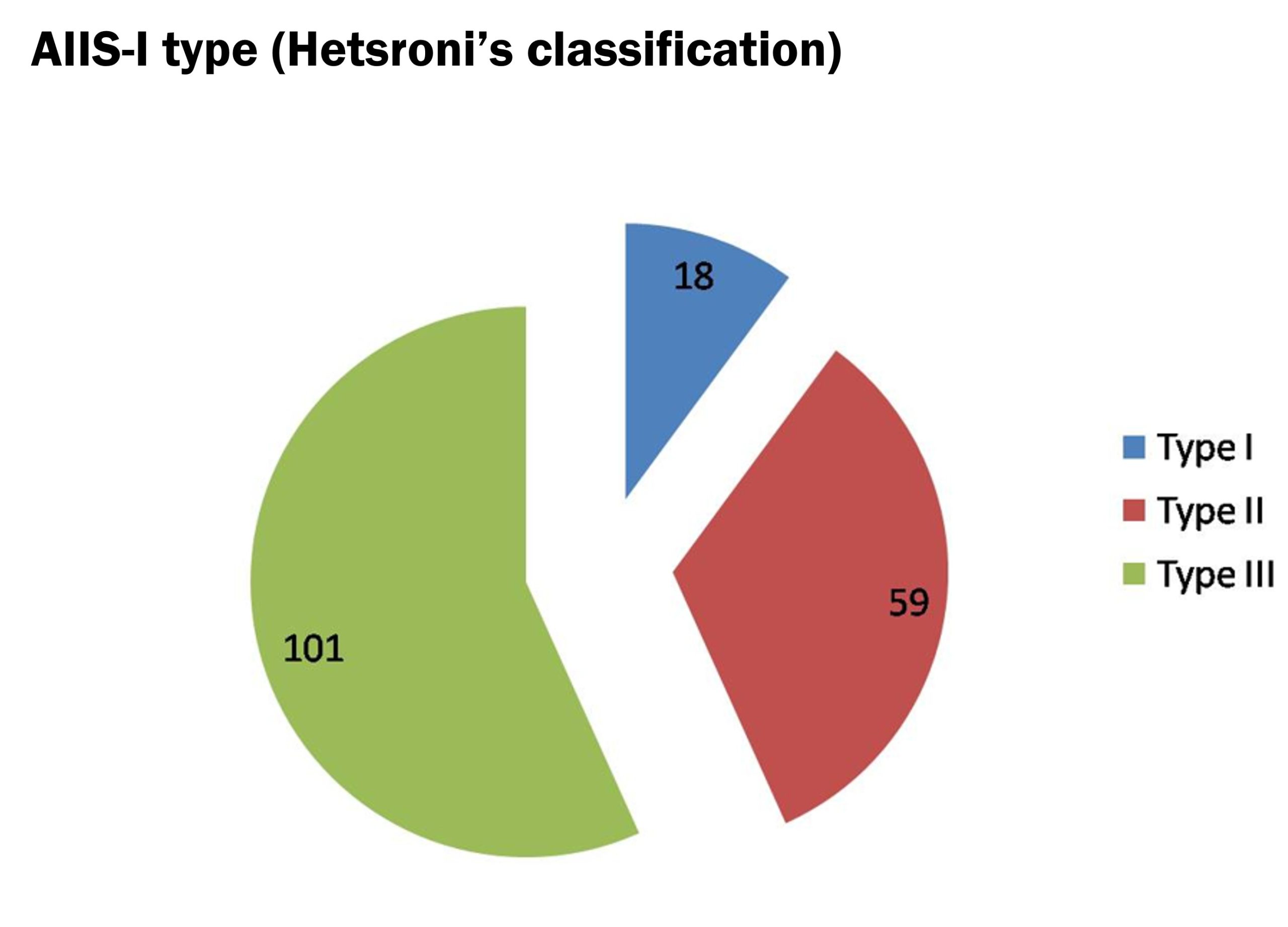
By the analysis of the series of patients managed by the members of the Hip Committee of SIAGASCOT, the prevalence of AIIS-I in a population of patients affected by GPS and operated for FAI in 10 years (minimum follow-up of 2 years) was 3.19% (178 cases – Figure 1). All patients reported symptoms related to FAI; no patients with AIIS-I alone were treated. The overall mean age at the time of surgery was 29.45 (range: 15-56), with the majority being male patients (153 vs. 25). According to Hetsroni’s classification for plain radiography, AIIS-I cases were assigned to the following types: type I – 18 cases, type II – 59 cases, and type III – 101 cases (Figure 2). The diagnostic evaluation used by surgeons was also based on CT/3D-CT scan and MRI/ArthroMRI, with the following combination: 84 cases diagnosed by X-rays and Arthro-MRI (46.9%), 65 with X-rays and MRI (36.5%), 29 with X-rays, MRI/Arthro-MRI, and CT (16.2%). All results showed p > 0.05 between the FAI and FAI + AIIS-I groups.
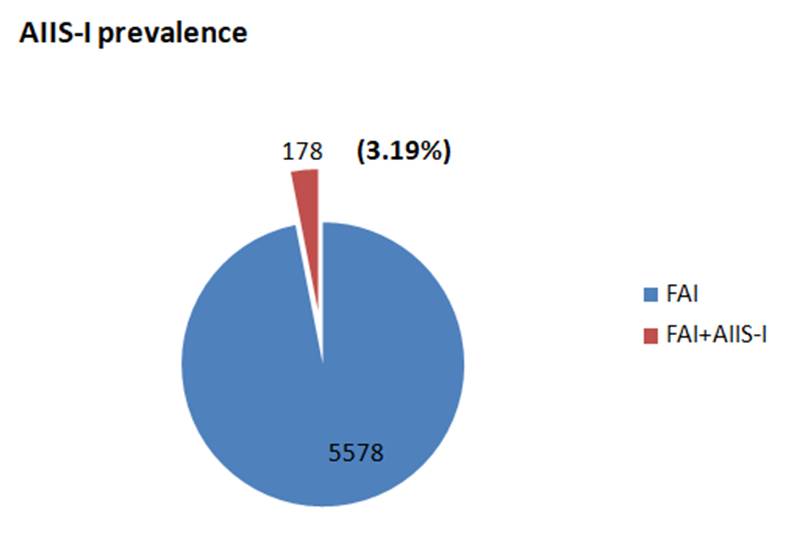
Figure 2. AIIS-I classification based on Hetsroni’s criteria.
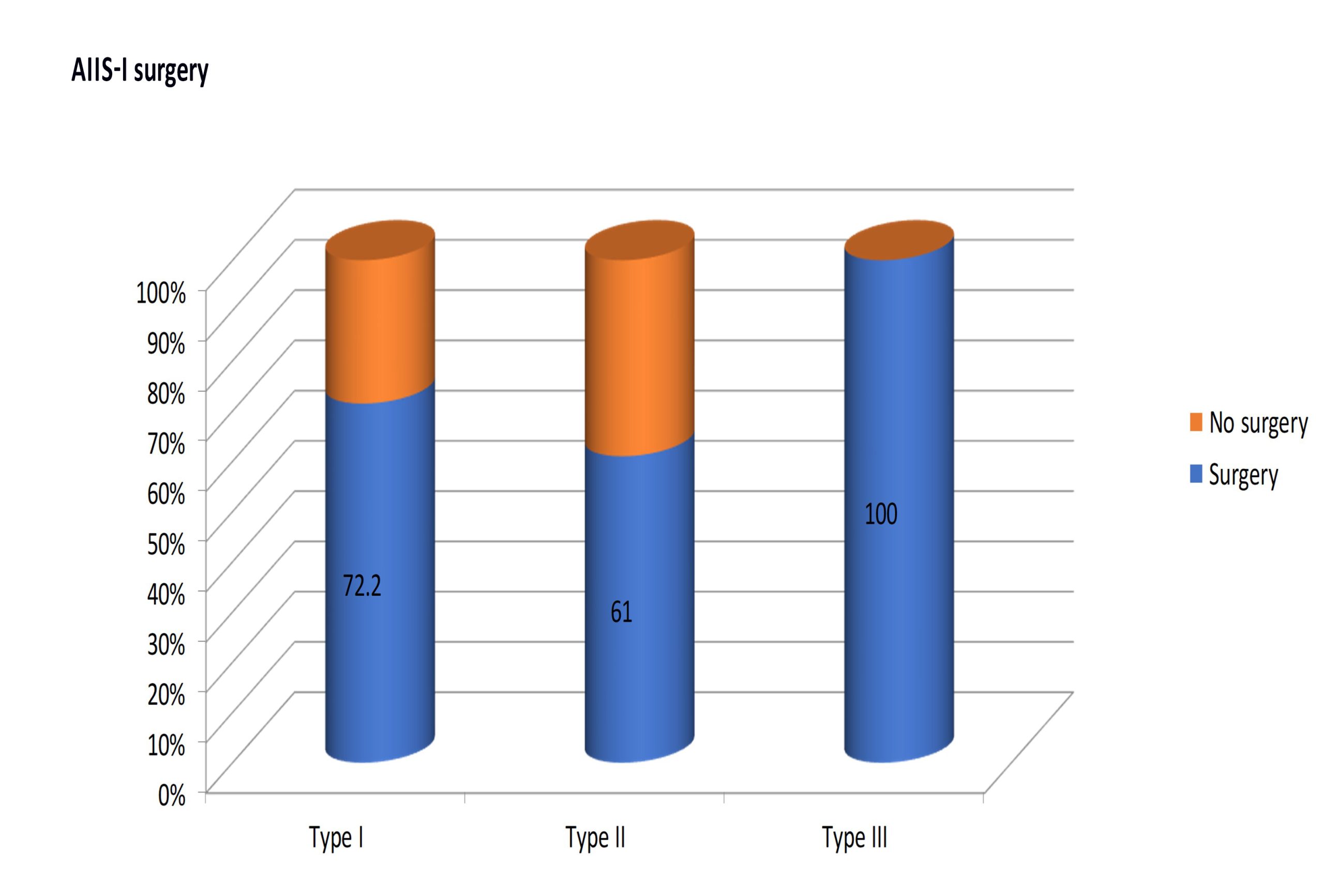
150 patients out of 178 (84.2%) underwent surgery for FAI and AIIS-I (Figures 3, 4, and 5), while the remaining subjects were managed only for FAI (Figures 6 and 7). Patients who were also operated for AIIS-I presented the following AIIS alteration according to Hetsroni’s classification (Figure 8): 13 patients with type I out of 18 (72.2%), 36 with type II out of 59 (61.0%), and 101 with type III out of 101 (100%).
Finally, in 57 hip arthroscopies, other procedures (other than FAI and/or AIIS-I osteoplasty) were performed: labral reinsertion or suture, labral debridement, microfractures for acetabular or femoral chondral lesions.
In this study, no complications were reported, except for two cases of local post-operative pain, managed with prolonged analgesic therapy (both patients affected by FAI alone).
No different post-operative rehabilitation protocols were proposed by surgeons for patients undergoing hip arthroscopy, both for FAI and AIIS-I, than for those treated only for FAI; similarly, no specific approach in return-to-sport programs was adopted for the athletic recovery of patients after FAI + AIIS-I osteoplasty than for those treated only for FAI.
Figure 3. A 24-year-old male professional soccer player affected by right groin pain syndrome who underwent surgery for FAI and AIIS-I. Plain radiographic studies show Cam-FAI and type II AIIS-I in “true AP” (a), Dunn 45° (b), 90° (c), and “false profile” (d) views.
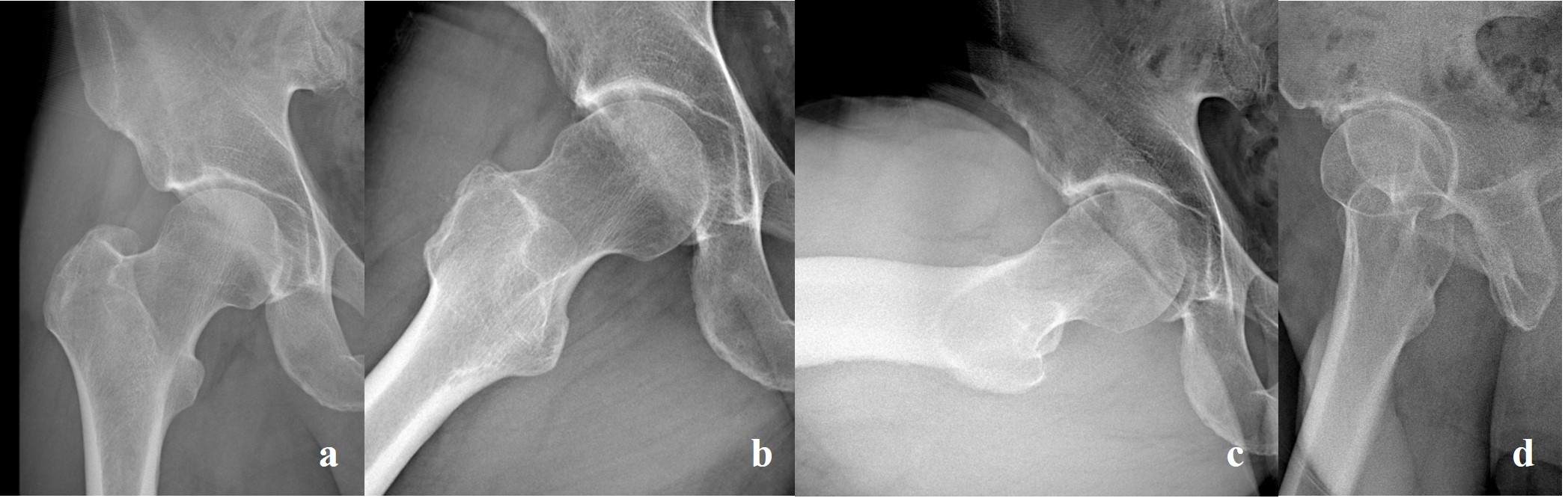
Figure 4. A 34-year-old male professional snowboarder with a previous rectus femoris lesion and moderate FAI: plain radiographic (a) and CT/3D CT scan (b) studies showing an acquired type III AIIS-I; arthroscopic treatment (c) and post-operative X-rays (d).
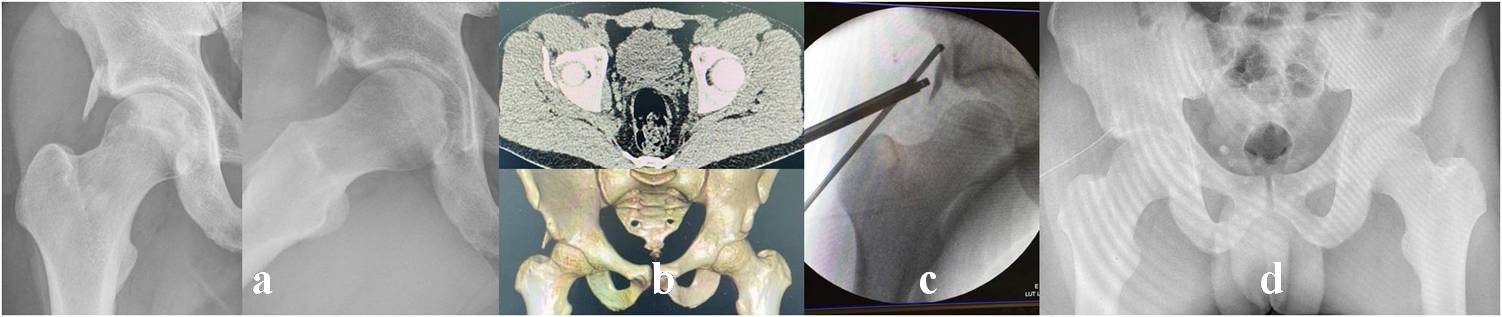
Figure 5. Arthrotomic treatment of a symptomatic FAI and type III right AIIS-I in a 15-year-old professional rugby player. Pre-operative plain radiography (a) and 3D-CT scan (b); intra-operative (c) and post-removal (d) images; X-rays after surgery (e).

Figure 6. Number and percentage of AIIS-I procedures performed on the overall study population (178 patients). Significance: p < 0.05.
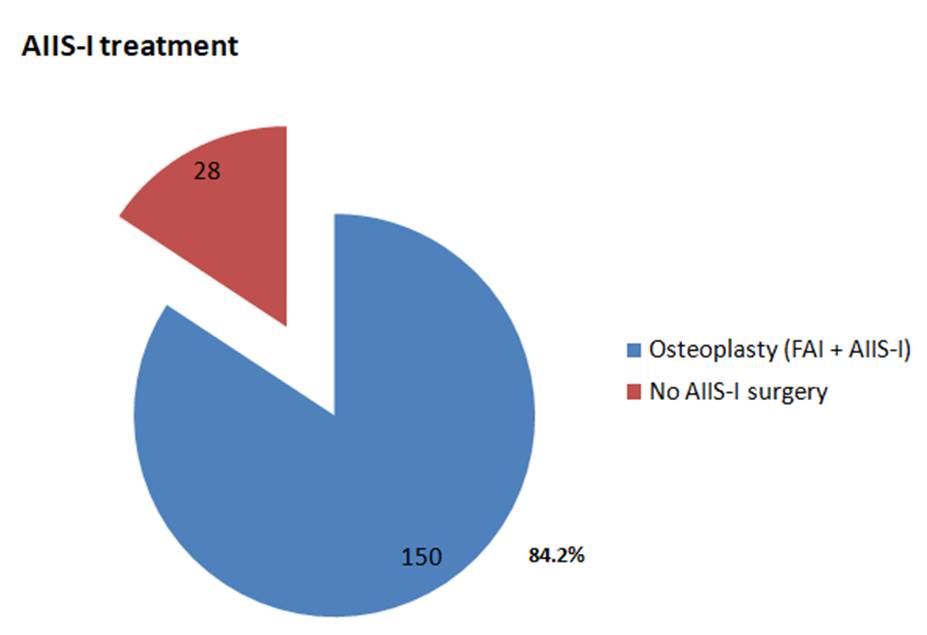
Figure 7. A 27-year-old non-professional female runner affected by left hip pain: plain radiographic study shows a minimal Cam-FAI and type I AIIS-I in “true AP” (a), Dunn 45° (b), 90° (c), and “false profile” (d) views. The patient was scheduled for surgery, but underwent only FAI treatment.

Figure 8. Numbers and percentages of AIIS-I operated cases related to Hetsroni’s classification. Significance: p < 0.05.
Discussion
AIIS-I is a form of impingement marked by a bony alteration that may cause additional symptoms in active patients with FAI, usually young and engaged in sports activities1,5,7-9: large AIIS deformities, as type III following Hetsroni’s classification, may require surgical treatment5,9. Other minimal or mild abnormalities should be assessed and managed by surgeons on a case-by-case basis, depending on their experience, the level of activity, or the type of sports each patient participates in9,10.
As a result of this retrospective observational study involving high-volume hip-preservation surgeons at a national level, the prevalence of AIIS-I in subjects operated for FAI was 3.19%. Moreover, 84.2% of patients with AIIS alterations underwent surgical management. These findings confirm that the phenomenon is not rare, but also not as common as reported in a few other reports1,5,7. However, when present as a significant deformity, AIIS-I may warrant surgical osteoplasty5,9. It needs attention and further study that 100% and 72.2% of patients presenting type III and I AIIS-I deformities, respectively, were surgically treated, while only 61% of type II were operated. This may be linked to the limited recognition of AIIS-I as the actual source of symptoms compared to FAI, even among experienced surgeons, or to the small amount of impingement caused by this deformity during arthroscopy.
In the literature, considering the post-operative improvements in various clinical scores and/or muscular strength tests reported by several authors, it is questionable whether these outcomes are related to the actual effect of AIIS decompression combined with FAI elimination5,9. It may be just related to the weakness of the hip flexors or to pain associated with the limiting function typically seen with FAI5,9. An undefined point may arise regarding the relatively high reoperation rate after hip arthroscopies and persistent pain due to untreated AIIS-I, in particular for minimal or mild AIIS deformities5,8-10. No reoperations for recurrence or persistence of groin pain syndrome were reported in the present study.
On the other hand, it is reasonable to expect that type III deformities are correlated with symptoms and should be surgically managed4,8,10,12.
Finally, there are very few case reports13-16 demonstrating the outcome in terms of return to sport after AIIS-I surgical decompression in high-level sport subjects. The authors reported good functional outcomes in patients undergoing AIIS-I decompression with FAI treatment. Only one study was a case series with level IV evidence, including 33 female patients who underwent arthroscopic AIIS decompression alone, without any concurrent FAI treatment16. The minimal clinically important difference (MCID) at 1-year follow-up had been achieved in the majority of patients: of note, all patients were also treated for labral tear, so further studies are needed to evaluate the true effectiveness and the objective outcomes of AIIS-I treatment alone or other surgical procedures16. In the present study, no specific aspect has emerged in rehabilitation or athletic recovery for patients undergoing combined FAI and AIIS-I osteoplasty. As reported in the literature, post-operative protocols are mostly related to FAI than to AIIS-I.
The present study has some limitations: firstly, it is a retrospective analysis of the last 10 years of clinical experience of the members of a national Committee on hip conservative surgery, and some cases of AIIS-I before this temporal window may have been lost. As the second point, no standardized evaluations were reported during the diagnostic process, which consequently influenced the choice of treatment. Finally, the relatively low percentage of treated type II deformities is hardly justifiable, showing the different interpretation of the clinical impact of AIIS-I by each surgeon for each patient.
Conclusions
AIIS-I is an uncommon form of hip impingement alteration that should be taken into account by dedicated hip preservation surgeons, mostly in cases of moderate/severe deformity or in high-level athletes complaining of groin pain. The diagnostic evaluation has been performed variably to date, but AIIS-I may be confirmed during surgery. Given that symptoms related to this condition are usually less evident than FAI, several cases of AIIS-I are underestimated and undertreated. Finally, to date, no specific rehabilitation programs or return-to-sport protocols have been proposed for athletes who have undergone surgery for FAI and AIIS-I.
Conflict of Interest
The authors declare no conflict of interest or any issue that may have induced bias in the writing of the paper.
Authors’ Contributions
All authors have equally participated and contributed to the writing, development, and analysis of data.
Ethics Approval
Ethical approval was obtained from the Ethical Committee of Careggi University Hospital, Florence, Italy (CEAVC_Prot. 24116 on 26/11/2024).
Informed Consent
All patients in all affiliations have been informed and have given their consent to the retrospective use of non-sensitive data for scientific purposes.
AI Disclosure
No AI-related tools or any form of generative artificial intelligence were adopted for writing the manuscript.
Funding
No funding was provided for any aspect of this independent study at any patient enrollment site.
ORCID ID
C. Carulli: 0000-0002-0845-7940
A. Aprato: 0000-0002-2514-4719
F. Randelli: 0000-0002-7643-0512
L. Perticarini: 0000-0002-7318-3878
A. Costantini: 0000-0002-0558-3714
References
- Kobayashi N, Kamono E, Yamamoto Y, Yukizawa Y, Honda H, Takagawa S, Misumi T, Inaba Y. Imaging Diagnosis, Prevalence, and Clinical Outcomes of Arthroscopic Surgery for Anterior Inferior Iliac Spine Impingement: A Systematic Review and Meta-analysis. Orthop J Sports Med 2022; 10: 23259671221131341.
- Carton P, Filan D. Anterior Inferior Iliac Spine (AIIS) and Subspine Hip Impingement. Muscles Ligaments Tendons J 2016; 6: 324-336.
- Larson CM, McGaver RS, Collette NR, Giveans MR, Ross JR, Bedi A, Nepple JJ. Arthroscopic Surgery for Femoroacetabular Impingement in Skeletally Immature Athletes: Radiographic and Clinical Analysis. Arthroscopy 2019; 35: 1819-1825.
- Reboli M, Aprato A, Vittori J, Olivero M, Bosco F, Massè A. Reevaluation of the surgical indications for anterior inferior iliac spine avulsion fractures in an acute setting – A narrative review of the current literature. J Orthop 2023; 38: 20-24.
- Ross JR, Larson CM, Adeoye O, Kelly BT, Bedi A. Residual deformity is the most common reason for revision hip arthroscopy: a three-dimensional CT study. Clin Orthop Relat Res 2015; 473: 1388-1395.
- Westermann RW, Schaver AL, Larson CM. Capsule-Preserving Approach to Arthroscopic Decompression of the Anterior Inferior Iliac Spine. Arthrosc Tech 2021; 10: e815-e819.
- Hetsroni I, Poultsides L, Bedi A, Larson CM, Kelly BT. Anterior inferior iliac spine morphology correlates with hip range of motion: a classification system and dynamic model. Clin Orthop Relat Res 2013; 471: 2497-2503.
- Ilizaliturri VM Jr, Arriaga Sánchez R, Suarez-Ahedo C. Arthroscopic Decompression of a Type III Subspine Impingement. Arthrosc Tech 2016; 5: e1425-e1431.
- Schaver AL, Leary SM, Henrichsen JL, Larson CM, Westermann RW. Outcomes of Arthroscopic Decompression of the Anterior Inferior Iliac Spine: A Systematic Review and Meta-analysis. Am J Sports Med 2023; 51: 1096-1105.
- Tateishi S, Onishi Y, Suzuki H, Takahashi M, Shiraishi J, Larson CM, Uchida S. Arthroscopic anterior inferior iliac spine decompression does not alter postoperative muscle strength. Knee Surg Sports Traumatol Arthrosc 2020; 28: 2763-2771.
- Ricciardi BF, Fields K, Kelly BT, Ranawat AS, Coleman SH, Sink EL. Causes and risk factors for revision hip preservation surgery. Am J Sports Med 2014; 42: 2627-2633.
- Hapa O, Bedi A, Gursan O, Akar MS, Guvencer M, Havitcioglu H. Anatomic footprint of the direct head of the rectus femoris origin: cadaveric study and clinical series of hips after arthroscopic anterior inferior iliac spine/subspine decompression. Arthroscopy 2013; 29: 1932-1940.
- De Sa D, Alradwan H, Cargnelli S, Thawer Z, Simunovic N, Cadet E, Bonin N, Larson C, Ayeni OR. Extra-articular hip impingement: a systematic review examining operative treatment of psoas, subspine, ischiofemoral, and greater trochanteric/pelvic impingement. Arthroscopy 2014; 30: 1026-1041.
- Pan H, Kawanabe K, Akiyama H, Goto K, Onishi E, Nakamura T. Operative treatment of hip impingement caused by hypertrophy of the anterior inferior iliac spine. J Bone Joint Surg Br 2008; 90: 677-669.
- Larson CM, Kelly BT, Stone RM. Making a case for anterior inferior iliac spine/subspine hip impingement: three representative case reports and proposed concept. Arthroscopy 2011; 27: 1732-1737.
- Nwachukwu BU, Chang B, Fields K, Rinzler J, Nawabi DH, Ranawat AS, Kelly BT. Outcomes for Arthroscopic Treatment of Anterior Inferior Iliac Spine (Subspine) Hip Impingement. Orthop J Sports Med 2017; 5: 2325967117723109.
To cite this article
Subspine impingement: a national multicenter retrospective observational study on prevalence, diagnosis, treatment, rehabilitation, and athletic recovery
JOINTS 2026;
4: e2013
DOI: 10.26355/joints_20265_2013
Publication History
Submission date: 16 Jan 2026
Revised on: 19 Mar 2026
Accepted on: 06 May 2026
Published online: 14 May 2026