JOINTS 2026;
4: e2116
DOI: 10.26355/joints_202606_2116
Pulsed electromagnetic fields in muscle and tendon injuries: a narrative review of preclinical and clinical evidence
Topic: New Technologies
Category: Narrative Review
Abstract
Clinical biophysics is an interdisciplinary field that applies quantitative physical methods to study how non-ionizing physical stimuli interact with and modulate living systems. This field integrates fundamental concepts from pharmacology to characterize the parameters of physical agents, understand their mechanisms of action and the metabolic pathways they activate, and evaluate their therapeutic efficacy in addressing specific pathological conditions. Clinical biophysics introduces a new pharmacological approach that replaces chemical agents with physical stimuli – such as specific frequencies, amplitudes, waveforms, and exposure durations – to modulate cellular functions. The cell membrane serves as the primary interface for these biophysical effects. Among the key modalities explored within this framework are pulsed electromagnetic fields (PEMFs), widely utilized for promoting bone and cartilage regeneration and currently under investigation for their applications in muscle and tendon healing. Promising outcomes have been reported across both in vitro and in vivo studies. The specificity and selectivity required for treating distinct pathological conditions depend on the careful modulation of physical parameters, allowing for tailored therapeutic protocols. PEMF stimulation interacts with adenosine and other mechanoreceptors to activate early genes like c-fos, promoting anabolic differentiation influenced by the surrounding extracellular microenvironment. Hence, PEMF therapy should not be viewed as an indiscriminate, universal solution but rather as a highly adaptable therapeutic tool that, by adjusting stimulation parameters to the specific needs of each tissue, can selectively drive anabolic processes by activating early differentiation mechanisms and their interactions with the local extracellular matrix. The aim of the present review is to offer an in-depth overview of the mechanisms by which PEMFs exert their effects and summarize recent advances from preclinical and clinical studies focused on muscle and tendon injuries, showing their promising potential for orthopedic pathologies.
Introduction
The interaction between electric and magnetic forces generates electromagnetic fields (EMFs), dynamic phenomena characterized by variable signal frequencies, waveforms, and intensities, each capable of producing either positive or negative biological outcomes. In the medical field, EMFs have found application both diagnostically and therapeutically, with a growing body of evidence highlighting their ability to influence cellular behavior and promote tissue regeneration1. By acting at the cell membrane level, EMFs can modulate cellular functions and disturb or restore homeostatic processes. Their dual nature, offering therapeutic promise while posing potential biological risks, necessitates continuous monitoring and sustained investigative efforts. Advancing the understanding of EMF-biological interactions is pivotal for maximizing therapeutic outcomes while minimizing potential adverse effects2.
Within the broader family of EMFs, pulsed electromagnetic fields (PEMFs) have attracted particular attention as therapeutic tools. These noninvasive and economically accessible treatments have demonstrated efficacy across multiple pathological contexts3,4. PEMFs are capable of modulating key cellular events, such as proliferation, differentiation, apoptosis, regulation of the cell cycle, and interactions with the extracellular matrix. Through these mechanisms, PEMFs can alter cell physiology and initiate extensive biological cascades5. Furthermore, PEMF exposure can influence cellular behavior indirectly by modulating signal transduction pathways, including A2A adenosine receptors and the mitogen-activated protein kinase/extracellular signal-regulated kinase (MAPK/ERK) pathway, while also restoring cellular homeostasis. Biological mediators such as calcium ion flux, nitric oxide signaling, and growth factor release have been implicated in the cellular responses elicited by PEMFs6. These mechanisms promote the upregulation of regenerative and tendon-related markers, including scleraxis, vascular endothelial growth factor (VEGF-A), and collagen type I, while also enhancing the release of interleukin (IL)-6, IL-10, and transforming growth factor-beta (TGF-β), together with increased elastin and fibronectin production in tendon cells.
The biological effectiveness of PEMFs depends critically on technical parameters including signal waveform, intensity, frequency, and exposure dose7. Preclinical research aimed at optimizing these variables is vital for translating PEMF therapy into reliable clinical interventions. Additionally, it is important to recognize that not all cell types respond uniformly to PEMF exposure, underscoring the need for careful dosimetry and a nuanced understanding of the complex interactions between physical stimuli and biological systems. As in the field of pharmacology, dose-response relationships constitute a fundamental aspect of developing safe and effective clinical applications of PEMFs8.
Biophysics serves as a bridge between physics and biology, applying physical principles and methodologies to explore the behavior of biological systems. It specifically focuses on how non-ionizing physical stimuli – such as electrical, magnetic, and mechanical forces – interact with biological tissues to alter their functional states, a process termed biophysical stimulation. In clinical applications, biophysical stimulation can function as a primary therapeutic strategy aimed at reinforcing reparative and anabolic activities within tissues9. Moreover, when used alongside pharmacological agents or growth factors, biophysical stimulation can enhance therapeutic outcomes while simultaneously reducing drug dosages and limiting adverse effects, thereby positioning itself as a powerful adjunct to traditional medical treatments.
The aim of this review is to delve into the role of PEMF-based biophysical stimulation in regenerative medicine, considering both preclinical and clinical evidence, with particular emphasis on its applications in promoting muscle and tendon repair in sports medicine and orthopedic contexts.
Methodology
Eligible studies included original experimental, preclinical, and clinical research evaluating PEMF interventions in skeletal muscle and tendon. Both in vitro and in vivo studies were considered when they explored biological mechanisms, cellular responses, tissue healing, angiogenesis, myogenesis, tenogenesis, osteogenesis, chondrogenesis, or functional outcomes associated with electromagnetic stimulation. Clinical studies involving human participants with musculoskeletal disorders, sports injuries, osteoarthritis, tendon pathology, postoperative rehabilitation, or muscle dysfunction were also included if PEMF therapy was used as a therapeutic intervention. Review articles, systematic reviews, and meta-analyses were retained for background synthesis and contextual.
Biophysical Stimulation in Regenerative Medicine for Muscular Lesions
As one of the largest organs in the human body, skeletal muscle plays a critical role in enabling both respiration and movement. Its intricate structural organization grants it an extraordinary capacity for regeneration, a function predominantly mediated by resident muscle stem cells10. Nevertheless, this innate reparative ability may become impaired in the context of severe injury. In response to such limitations, recent preclinical investigations have increasingly focused on applying biophysical stimulation techniques to promote muscle repair.
Preclinical Evidence
The intricate anatomical organization of skeletal muscle enables the precise generation of contractile forces essential for both respiration and movement11. This contractile function is attributed to the structural arrangement of myofibers, which are formed through the fusion of myoblasts into multinucleated myotubes. In addition to its mechanical capabilities, skeletal muscle is distinguished by a remarkable regenerative capacity, particularly following minor injuries12. This regenerative potential largely depends on the activity of muscle stem cells, known as satellite cells, which reside in a quiescent state and become activated when repair is required, ensuring rapid recovery and the preservation of muscle function. However, in the presence of severe trauma or pathological conditions, this intrinsic self-repair mechanism can be significantly impaired13.
Beyond satellite cells and myoblasts, adult skeletal muscle also hosts a variety of progenitor cell populations with high myogenic potential. These include CD133+ progenitor cells, muscle-derived stem cells (MDSCs), multipotent perivascular progenitor cells, and muscle-derived side-population (SP) cells. Furthermore, multipotent cells capable of myogenic differentiation have been isolated from non-muscle tissues such as bone marrow, adipose tissue, and umbilical cord sources12-14.
Efforts in tissue engineering and regenerative medicine have extensively explored strategies to enhance the muscle healing response following injury, such as cell therapy, tissue engineering, and acellular scaffold implantation14. Cell therapy is a therapeutic approach involving the direct injection of exogenous myogenic progenitor cells into damaged muscle tissue. Among the most studied cell sources is the stromal vascular fraction derived from adipose tissue, known for its capacity to differentiate into adipogenic, chondrogenic, osteogenic, and myogenic lineages15. This myogenic potential has been validated both through in vitro and in vivo studies16. Interestingly, after intramuscular administration, adipose-derived stem cells (ADSCs) have demonstrated the ability to suppress inflammation, promote angiogenesis, and restore dystrophin expression in a mouse model of muscular dystrophy17. Additionally, Kang et al18 reported that ADSC transplantation in a murine ischemic hindlimb model enhanced vascular density and reduced muscle atrophy at four weeks post-injury. Nevertheless, the clinical translation of cell therapy approaches has been challenged by issues such as poor cell survival, limited engraftment into host tissues, and complex regulatory hurdles19.
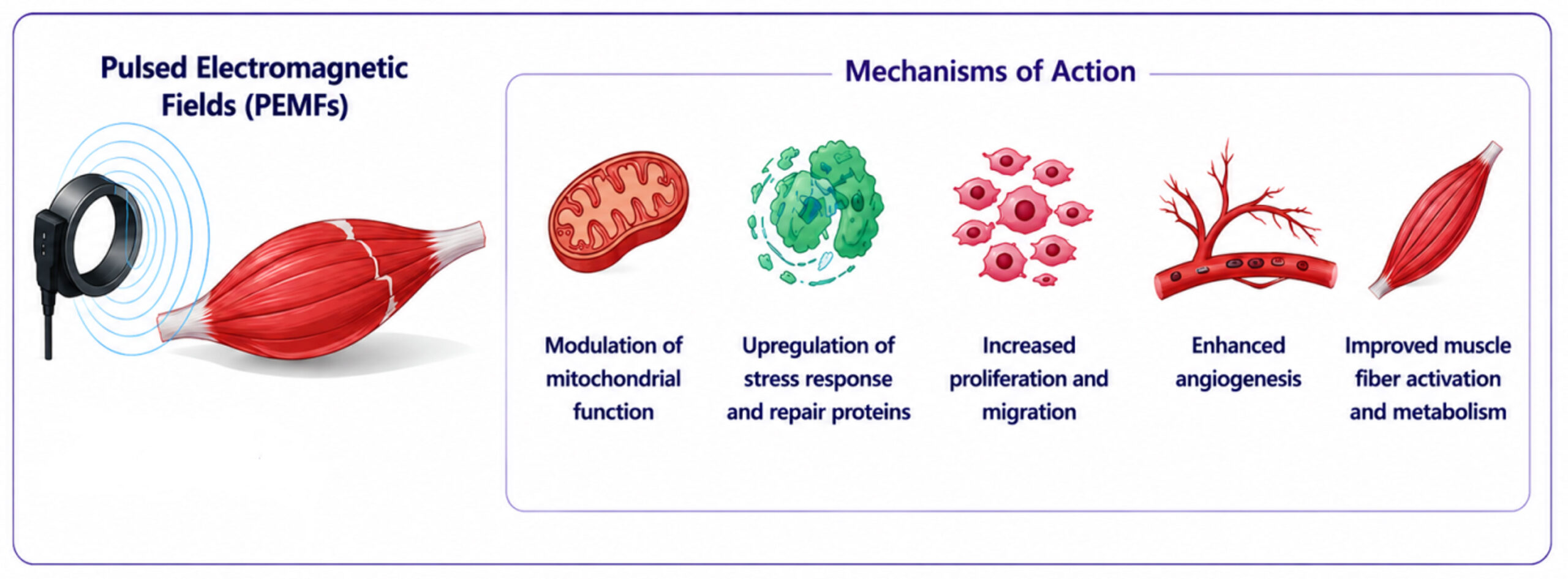
Emerging evidence20-22 suggests that biophysical stimulation represents a promising adjunctive strategy to enhance muscle regeneration, leveraging the intrinsic contractile properties of skeletal muscle. Various modalities, including mechanical stimulation, electrical stimulation, and their combined application, have been studied for their capacity to activate and support the regenerative niche within muscle tissue23. Although electrical stimulation and pharmacological interventions have historically dominated tissue regeneration research, both techniques are associated with notable limitations, prompting the search for alternative therapies. Within this context, PEMFs have garnered interest as a potential non-invasive method to stimulate skeletal muscle regeneration (Figure 1). The in vitro study from Maiullari et al24, demonstrated that PEMF exposure can facilitate muscle cell repair by upregulating proteins associated with cellular stress responses and damage repair mechanisms. Specifically, skeletal muscle cells (SkMCs) exposed to a 1.5 mT PEMF stimulus for four hours across two consecutive days exhibited increased proliferation without signs of apoptosis or metabolic dysfunction. Remarkably, PEMF-treated cells showed accelerated wound closure and enhanced migratory activity in scratch assays, indicating a facilitated regenerative response.
Clinical Evidence
Recent evidence suggests that PEMFs modulate mitochondrial function, thereby promoting regenerative processes and tissue repair25. Such properties are particularly relevant in post-operative rehabilitation scenarios, including recovery following anterior cruciate ligament reconstruction (ACLR). A randomized controlled clinical trial26 evaluated the impact of PEMFs during the post-operative phase of ACLR rehabilitation. Results demonstrated that patients receiving PEMF therapy exhibited superior improvements in quadriceps muscle strength compared to those undergoing standard rehabilitation alone. These functional gains were corroborated by imaging assessments, including ultrasound and magnetic resonance imaging (MRI), which confirmed increases in muscle volume. In a separate double-blind, placebo-controlled randomized trial27, the efficacy of PEMF in alleviating delayed onset muscle soreness (DOMS) was investigated in 30 healthy male participants. Primary endpoints included assessments of muscle pain, peak torque, median frequency (MDF), and electromechanical delay (EMD) during isometric contractions at 24-, 48-, and 72-hours following DOMS induction. PEMF therapy was associated with significant improvements in muscle pain perception, MDF, and EMD, reflecting accelerated recovery from physiological impairments. However, no significant advantage was observed over placebo regarding improvements in peak isometric torque. Further research assessed the influence of PEMF on muscle activation and metabolism during exercise in semi-professional cyclists. In a randomized crossover study, Trofè et al28 evaluated twenty athletes engaged in constant-load exercise sessions under active (ON) and inactive (OFF) PEMF stimulation conditions. During the load-free warm-up phase, active PEMFs significantly increased muscle activity. Additionally, higher blood lactate concentrations were recorded during PEMF exposure, suggesting an enhancement of glycolytic metabolic pathways. These findings indicate that PEMF stimulation can promote increased muscle fiber activation and metabolic responsiveness during low-intensity exercise.
The research works reviewed in this section are listed in Table 1.
| Study | Study design | Experimental model | PEMFs characteristics | Main results |
| Maiullari et al24 | In vitro | Skeletal muscle cells | 1.5 mT, 75 Hz
4 h for 2 days |
Increased proliferation and migration |
| Ong et al26 | RCT | Adult patients (aged 18-30) with unilateral anterior cruciate ligament injury | 1 mT, 15 Hz
10 minutes twice a week for 8 weeks |
Improved quadriceps muscle strength |
| Jeon et al27 | RCT | Healthy males (mean age 23.1) upon delayed onset muscle soreness (DOMS) induction | 0.2 T, 1 Hz
10 minutes for 4 days |
Reduced DOMS severity and shorter recovery time |
| Trofè et al28 | RCT | Male semi-professional cyclists (mean age 22.3) | 5 μT, 2 Hz
during 1 minute of warm-up + variable constant-load physical effort |
Increased muscle activity in the warm-up condition and blood lactate concentration |
Figure 1. PEMF therapy for muscular lesions. PEMF therapy promotes mitochondrial function, induces stress response, proliferation, migration, and angiogenesis, and improves muscle fiber activation and metabolism.
Biophysical Stimulation in Regenerative Medicine for Tendon Lesions
While PEMFs have long been explored for therapeutic applications in several fields, their widespread clinical adoption for the treatment of tendinopathies and tendon injuries remains an unmet objective. Tendon tissue represents one of the most recent frontiers for biophysical stimulation strategies. Although modern in vitro investigations have yielded promising results, it is noteworthy that a substantial, yet relatively under-recognized, body of clinical and preclinical research originating from the 1980s already suggested a potential role for PEMF therapy as a conservative treatment option for tendon pathologies.
Preclinical Evidence
The earliest preclinical investigation into the effects of PEMFs on tendon healing dates back to the 1980s, when Watkins et al29 created defects in the superficial digital flexor tendons of a horse model. Animals exposed to PEMF treatment for only two hours daily exhibited delayed maturation of the reparative tissue within the lesion. In the ensuing decades, research predominantly shifted toward small animal models, a transition likely driven by economic considerations and the enhanced reproducibility of experimental outcomes. In 1997, Lee et al30 demonstrated the beneficial role of PEMFs in a rat model of experimental Achilles tendonitis, where treatment was associated with reduced inflammation and a more complete restoration of the tendon’s histological architecture. Further evidence was subsequently provided by Strauch et al31, who investigated PEMF application following Achilles tendon transection and repair in rats. Their findings indicated a substantial increase (up to 69%) in the tensile strength at the repair site after three weeks compared to unstimulated controls. These observations began to suggest that PEMFs might accelerate tendon healing, opening the possibility for early rehabilitation protocols incorporating PEMF exposure in clinical practice.
The concept of accelerated tendon healing was further reinforced by Tucker et al32, who utilized a rat model of acute rotator cuff detachment and repair. Their work highlighted the capacity of PEMFs to enhance tendon-to-bone healing, evidenced by improved mechanical and histological tendon properties. Specifically, they observed an early increase in the elastic modulus (notably at 4-8 weeks post-injury), alongside cellular changes such as more rounded tenocyte morphology, suggestive of heightened metabolic activity, and better-organized collagen fibers within the tendon substance. This study represents a pivotal milestone in preclinical PEMF research. Similar trends were noted in the study conducted by Huegel et al33 which evidenced that in a bilateral rat supraspinatus injury model, enhanced tendon mechanical properties, including modulus and stiffness, and improved collagen organization were reported following PEMF exposure for up to six hours daily. Consistent findings were later confirmed by Dolkart et al34 using the same model, reinforcing the positive impact of PEMFs during the early stages of tendon healing. Mechanistic insights were further advanced by Huegel et al35, who identified that PEMF exposure promoted upregulation of bone morphogenetic protein 2 (BMP2) signaling, increased the expression of pro-osteogenic genes at the tendon-bone interface, downregulated genes associated with fibrotic healing, and induced anti-inflammatory shifts, such as the transition of macrophages from an M1 to an M2 phenotype. However, not all findings were uniformly positive. In a subsequent study, the same group36 reported that PEMFs failed to enhance healing in a rat Achilles tendon tear model (both complete tears with surgical repair and partial tears without repair) following up to three hours of daily stimulation. Differences in the anatomical and biomechanical nature of the lesions (Achilles tendon injuries being purely soft tissue, whereas supraspinatus injuries involve a tendon-bone interface) likely account for the observed discrepancies. These results highlight the necessity of more nuanced preclinical evaluations to clarify the contexts in which PEMF therapy is most effective. Interestingly, even in this model, partial-width Achilles tears exhibited early positive responses to PEMF exposure, suggesting that the timing and extent of injury may influence therapeutic outcomes. Moreover, the rapid intrinsic healing capacity of rodent models may underestimate the potential clinical impact of PEMF therapy in humans.
Recent studies have renewed interest in PEMF application for Achilles tendinopathy. Perucca Orfei et al37 demonstrated an anabolic effect of PEMFs administered for eight hours daily. Using a type I collagenase-induced tendinopathy model, they found that PEMF exposure during the mid-acute phase (7-14 days post-induction) significantly improved collagen fiber architecture, restored normal cell morphology, and reduced inflammatory infiltrates. Supporting these findings, Uzun et al38 conducted a rabbit model study involving Achilles tendon tear and repair, applying PEMFs for 21 days post-surgery. Their results indicated effective tendon recovery, reinforcing the regenerative potential of PEMFs even though the precise molecular mechanisms remain incompletely understood. The effects of PEMFs on tendons are summarized in Figure 2.
In Vitro Modern Evidence
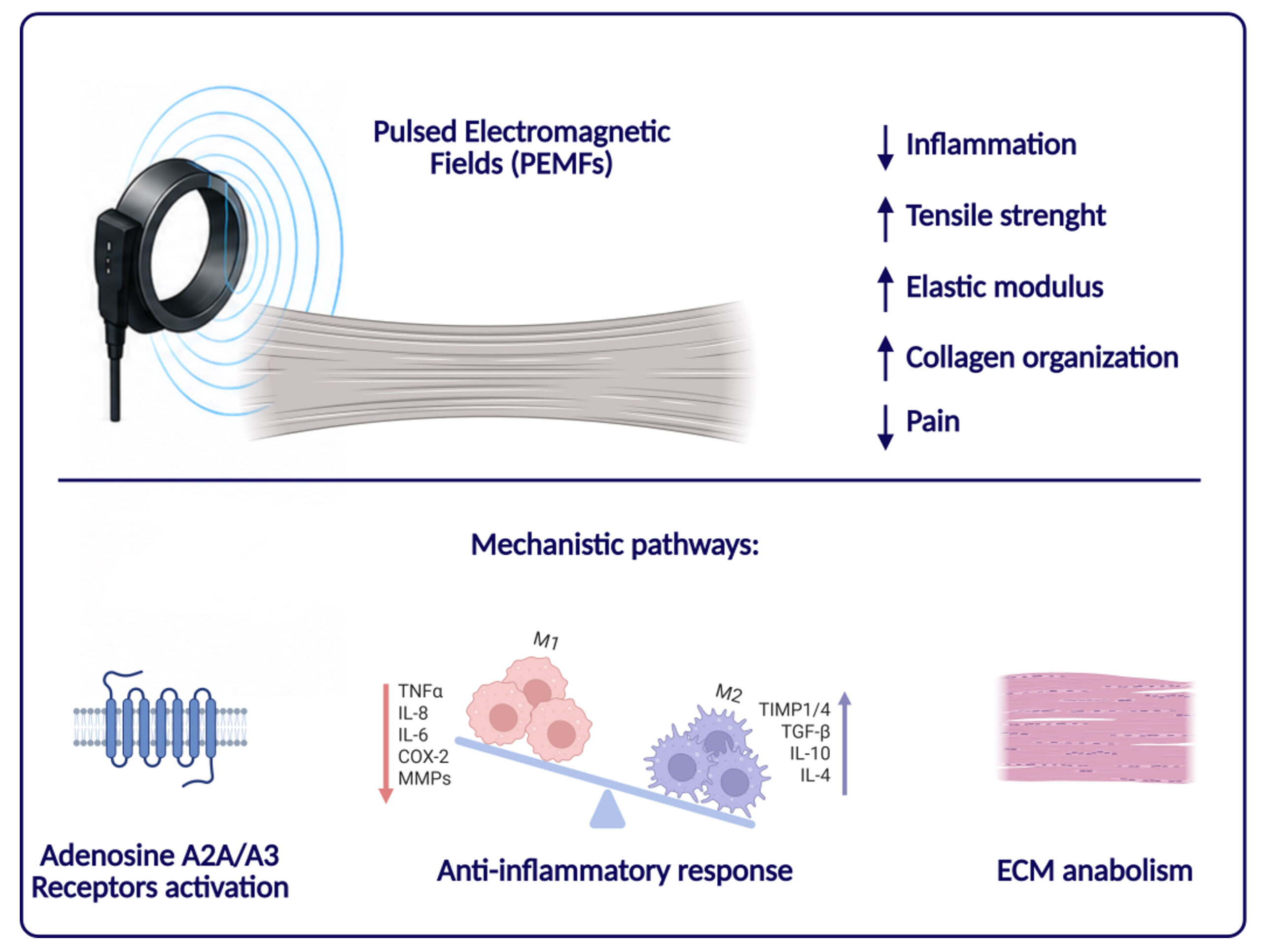
Despite the pre-clinical evidence supporting the use of PEMF, a detailed understanding of PEMF’s specific effects on tendon metabolism remains relatively limited39. In vitro studies have thus become a critical avenue for elucidating the cellular and molecular changes triggered by PEMF exposure, particularly concerning receptor activation and gene expression profiles. Rosso et al40 have highlighted several key mechanistic pathways (Figure 2):
- Adenosine receptors A2A and A3 activation:
In an experimental model involving tendon cells exposed to PEMFs for 48 hours alongside IL-1β stimulation, Colombini et al41 observed increased surface expression and ligand affinity of the A2A receptor. This upregulation was associated with a pronounced anabolic and reparative cellular response, characteristic of the early inflammatory phase of tendon healing, including elevated secretion of IL-6 and prostaglandin E2 (PGE2) and enhanced expression of the tenogenic markers scleraxis (SCX) and collagen type III alpha 1 (COL3A1). Complementary studies by de Girolamo et al42,43 further reported an upregulation of anti-inflammatory and pro-regenerative factors such as IL-10, vascular endothelial growth factor (VEGF-A), and transforming growth factor-beta (TGF-β) under PEMF stimulation.
- Upregulation of anti-inflammatory genes via the mitogen-activated protein kinase/extracellular signal-regulated kinase-1/2 (MAPK/ERK1/2) pathway:
Vinhas et al44,45 explored the anti-inflammatory potential of PEMFs using magnetically assisted cell sheets composed of human tendon-derived cells and magnetic nanoparticles exposed to IL-1β. Their findings demonstrated that brief PEMF treatment suppressed the expression of pro-inflammatory cytokines [IL-6, tumor necrosis factor-alpha (TNF-α), IL-8] and enzymes [cyclooxygenase-2 (COX-2), matrix metallopeptidase-1, -2, -3 (MMP-1, MMP-2, MMP-3)], while simultaneously enhancing the expression of anti-inflammatory mediators such as IL-4, IL-10, and tissue inhibitor of metalloproteinases-1 (TIMP-1)46. Supporting these observations, Gehwolf et al47 identified increased expression of IL-1 receptor type 2 (IL-1R2), a decoy receptor that modulates IL-1β signaling, following PEMF exposure, suggesting a significant immunomodulatory role.
- Promotion of extracellular matrix (ECM) anabolism:
Recent work by Marmotti et al48,49 revealed that prolonged PEMF stimulation (21 days) exerted strong anabolic effects on tenocytes48 or tendon explants49 derived from hamstring grafts used in anterior cruciate ligament reconstruction. Their study highlighted not only enhanced tenogenic differentiation but also upregulation of collagen type VI, a key ECM component with mechano-sensing functions. Similar anabolic responses were reported after exposing umbilical cord-derived mesenchymal stem cells to PEMFs50, supporting the hypothesis proposed by Viganò et al51 that mesenchymal precursor cells are important therapeutic targets of biophysical stimulation strategies. Furthermore, Liu et al52 demonstrated that PEMF exposure induced a marked anabolic gene expression profile in human rotator cuff tenocytes, but only under inflammatory conditions induced by IL-1β stimulation. Specifically, PEMF treatment led to significant upregulation of collagen I, TGF-β1, platelet-derived growth factor subunit B (PDGFb), BMP12, and TIMP4, highlighting its potential to enhance tendon repair processes within an inflammatory microenvironment, such as that present in the early postoperative period following rotator cuff repair.
Clinical Evidence
Since 1984, PEMFs have demonstrated promising therapeutic effects in the management of tendinopathies. In a pivotal pilot study, Binder et al53 conducted a double-blind randomized controlled trial focusing on persistent rotator cuff tendinitis, where they reported favorable outcomes following PEMF treatment. Building upon these early findings, subsequent clinical investigations explored the utility of PEMFs across various tendinopathies. In 1985, Devereaux et al54 evaluated the effects of PEMFs in patients with chronic lateral humeral epicondylitis; however, no significant clinical improvements were detected in their cohort. Conversely, in 2007, Uzunca et al55 demonstrated that PEMF therapy, when compared to corticosteroid injections and sham PEMF, significantly reduced pain during rest, activity, and nighttime in patients with lateral epicondylitis (“tennis elbow”), thereby providing stronger clinical evidence for the analgesic benefits of PEMF application in tendinous disorders. Further support for the therapeutic potential of PEMFs was later provided by Osti et al56, who showed that PEMF treatment in the early postoperative period following rotator cuff repair significantly reduced pain, decreased analgesic consumption, and improved joint stiffness. Although these benefits were apparent in the short term, no significant differences in outcomes between treated and untreated groups were observed at the two-year follow-up, suggesting that PEMFs may primarily exert an early acceleration of the healing process rather than affecting long-term outcomes. Additional confirmation of PEMF efficacy was obtained through a study conducted by Klüter et al57, who combined high-energy PEMF therapy with extracorporeal shock wave therapy (ESWT) in the conservative management of rotator cuff tendinopathy. Their results demonstrated significantly greater improvements in pain and functional outcomes after 24 weeks in patients receiving the combined treatment compared to those receiving ESWT alone, reinforcing the notion that PEMFs may provide clinical benefit even without surgical intervention. Nevertheless, some inconsistency remains in the literature. A more recent study58 failed to demonstrate a significant additional benefit of PEMF therapy when combined with diathermy [ultrasound (US)] and transcutaneous electrical nerve stimulation (TENS) compared to US and TENS alone, a result that may be attributed to the limited PEMF exposure time (25 minutes per session, five sessions per week for two weeks) used in that protocol. Emerging research continues to explore the broader potential of PEMFs in tendinopathy management. A 2023 investigation conducted by researchers at the Chinese University of Hong Kong proposed the use of PEMFs as an adjunctive therapy to eccentric exercise for the treatment of Achilles tendinopathy59. This ongoing prospective, randomized, double-blinded, placebo-controlled trial suggests that PEMF exposure may improve pain relief and enhance tendon mechanical properties, potentially augmenting the therapeutic response to standard eccentric exercise protocols. Should these findings be confirmed, PEMF therapy could represent a safe and effective conservative strategy for managing Achilles tendinopathy.
The research works reviewed in this section are listed in Table 2.
| Study | Study design | Experimental model | PEMFs characteristics | Main results |
| Watkins et al29 | in vivo | Horse | 1.5 Hz
2 h/day for 2, 4, 8, 12 or 24 weeks |
Delayed the maturation and collagen type transformation |
| Lee et al30 | in vivo | Rat | 15 Hz or 46 Hz
15 minutes/day up to 28 days |
Better collagen alignment, reduced inflammation |
| Strauch et al31 | in vivo | Rat | 27.12-MHz
two 30-minute sessions/day for 3 weeks |
Increased tensile strength |
| Tucker et al32 | in vivo | Rat | 0.5 mT, 3.85 kHz
3 h/day up to 112 days |
Increased modulus and maximum stress, more rounded cells, suggesting metabolic activation |
| Huegel et al33 | in vivo | Rat | 1.19 mT, 3.85 or 40.85 kHz
1, 3, or 6 h/day for 16 weeks |
Improved collagen expression and organization, increased modulus |
| Dolkart et al34 | in vivo | Rat | 0.05-0.5 mT, 10 kHz
continuous up to 40 days |
Improved elasticity, collagen expression and organization |
| Huegel et al35 | in vivo | Rat | 1.10 mT, 3.85 kHz
1 h/day for 28 days |
Upregulated bone morphogenetic protein 2 signaling and pro-osteogenic genes,
decreased fibrotic healing response and inflammation |
| Huegel et al36 | in vivo | Rat | 1.19 mT, 3.85 kHz
1 h/day up to 6 weeks |
No significant differences |
| Perucca Orfei et al37 | in vivo | Rat | 1.5 mT, 75 Hz
8 h/day for 7 or 14 days |
Better fiber organization, decreased cell density, vascularity, and fat deposition, restored physiological cell morphology |
| Uzun et al38 | in vivo | Rabbit | 1 mT, 15 Hz
1 h/day for 4 weeks |
Increased maximum load, toughness and maximum stress, better fiber organization |
| Colombini et al41 | ex vivo | Human tendon cells | 1.5 mT, 75 Hz
for 48 h |
A2AAR modulation, increased COL3A1 expression and IL-33 secretion |
| de Girolamo et al42 | ex vivo | Human tendon cells | 1.5 mT, 75 Hz for 4, 8, or 12 h | Increased proliferation, tendon-specific marker expression, and release of anti-inflammatory cytokines and angiogenic factor |
| de Girolamo et al43 | ex vivo | Human tendon cells | 1.5 or 3 mT for 8 or 12 h | Increased proliferation, upregulation of SCX, VEGF-A and COL1A1 expression, reduction of COL3A1 expression, higher release of IL-1β, IL-6, IL-10 and TGF-β |
| Vinhas et al46 | ex vivo | Human tendon cells | 1.5, 4 or 5 mT, 5 or 17 Hz for up to 7 days | Decreased expression of IL-6, TNF-α, IL-8, COX-2, MMP-1, MMP-2, and MMP-3, increased expression of IL-4, IL-10, and TIMP-1 |
| Gehwolf et al47 | ex vivo | Rat tendon constructs | 82 mT, 2 Hz
60 min twice |
Extracellular matrix remodeling, negative regulation of apoptosis |
| Marmotti et al48 | ex vivo | Human tendon cells | 1.5 mT, 75 Hz | Increased expression of collagen type I and VI, scleraxis |
| Marmotti et al49 | ex vivo | Human tendon explants | 1.5 mT, 75 Hz | Increased expression of collagen type I and VI, scleraxis, mTOR, c-fos |
| Liu et al52 | ex vivo/in vitro | Human tendon cells/ C2C12 murine myoblasts | 3 h/day 2 weeks | Increased tenocyte gene expression and myoblast differentiation |
| Binder et al53 | RCT | Persistent rotator cuff tendinitis patients | For 8 weeks | Significant benefit during the first 4 weeks |
| Devereaux et al54 | RCT | Lateral epicondylitis patients | For a minimum of 8 weeks | No significant differences |
| Uzunca et al55 | RCT | Lateral epicondylitis patients | 6 mT, 25 Hz + 4.6 Hz
For 30 min, 15 sessions for 3 weeks |
Reduced pain during rest, activity and nighttime |
| Osti et al56 | RCT | Patients upon shoulder arthroscopy | Not available | Reduced postoperative pain, analgesic use and stiffness in the short term |
| Özdemir et al58 | RCT | Patients with supraspinatus tendon tear | 50 Hz
25 minutes/day, 5 days/week for 2 weeks |
No significant differences |
| Ko et al59 | RCT | Patients with Achilles tendinopathy | 1 mT, 10 kHz
10 minutes twice a week for 8 weeks |
Ongoing |
Scleraxis (SCX); vascular endothelial growth factor (VEGF-A); transforming growth factor-beta (TGF-β); interleukin (IL); tumor necrosis factor-alpha (TNF-α); cyclooxygenase-2 (COX-2); matrix metallopeptidase-1, -2, -3 (MMP-1, MMP-2, MMP-3); tissue inhibitor of metalloproteinases-1 (TIMP-1); mammalian target of rapamycin (mTOR); collagen type III alpha 1 (COL3A1); collagen type I alpha 1 (COL1A1); A2A adenosine receptor (A2AAR).
Figure 2. PEMF therapy for tendon lesions. PEMF therapy reduces inflammation and pain and promotes tensile strength, elastic modulus and collagen organization. PEMFs act through activation of Adenosine A2A and A3 receptors, upregulating anti-inflammatory genes via the MAPK/ERK1/2 pathway and promoting extracellular matrix anabolism. Created in https://BioRender.com
Discussion
Experimental evidence indicates that PEMFs can influence key cellular processes involved in muscle repair, including proliferation, migration, oxidative stress responses, and mitochondrial metabolism. Maiullari et al24 demonstrated that PEMF exposure promoted skeletal muscle cell proliferation and accelerated wound closure without inducing apoptosis or metabolic dysfunction, suggesting a favorable regenerative microenvironment. Similarly, clinical investigations in postoperative rehabilitation and sports medicine demonstrated improvements in quadriceps strength, muscle activation, and recovery from delayed-onset muscle soreness. These findings support the concept that PEMFs may enhance muscle performance and recovery not only through structural regeneration but also through metabolic and neuromuscular adaptations. Despite these encouraging observations, the current evidence regarding PEMF therapy for muscular lesions remains limited by substantial heterogeneity in stimulation protocols, exposure duration, field intensity, treatment timing, and outcome measures. Furthermore, many available studies involve relatively small cohorts or experimental models, limiting the generalizability of their findings. The exact molecular mechanisms underlying PEMF-mediated muscle regeneration also remain incompletely understood. Nonetheless, emerging evidence6,25,42,43,52 suggests that PEMFs may regulate intracellular signaling pathways associated with calcium flux, nitric oxide release, mitochondrial dynamics, and growth factor expression, ultimately contributing to restoration of cellular homeostasis and tissue repair.
The evidence supporting PEMF application in tendon healing appears comparatively more extensive and mechanistically characterized. Preclinical animal studies29-38,47 consistently demonstrated improvements in tendon mechanical properties, collagen organization, and tendon-to-bone healing following PEMF exposure. Importantly, several investigations35,37,41-45,52 identified anti-inflammatory and anabolic effects mediated through modulation of adenosine receptors, MAPK/ERK signaling, and cytokine expression. PEMFs were shown to promote tenogenic differentiation, increase expression of collagen-related genes, and suppress pro-inflammatory mediators such as IL-1β, TNF-α, and matrix metalloproteinases. These biological effects are particularly relevant considering the limited vascularity and slow intrinsic healing capacity of tendon tissue. Nevertheless, tendon-related studies36,54,58 also revealed inconsistencies that warrant careful interpretation. While beneficial effects were frequently observed in rotator cuff and tendon-to-bone healing models, some studies failed to demonstrate significant improvements in Achilles tendon injuries36, lateral humeral epicondylitis54 and supraspinatus tendon tear58. Such discrepancies likely reflect differences in tendon biology, biomechanical loading, injury chronicity, and the presence or absence of a tendon-bone interface. Moreover, the timing and dosage of PEMF exposure appear to critically influence therapeutic efficacy, emphasizing the need for standardized stimulation parameters. Clinical evidence remains promising but still insufficient to support definitive recommendations for routine practice. Early randomized controlled trials53,55,56,59 demonstrated reductions in pain, stiffness, and analgesic consumption in rotator cuff tendinopathy and postoperative rehabilitation settings. More recent studies have suggested potential synergistic effects when PEMFs are combined with established conservative approaches such as extracorporeal shockwave therapy57 or eccentric exercise59. However, long-term superiority over standard treatments has not been consistently demonstrated, and several studies remain limited by small sample sizes, short follow-up periods, and variability in treatment protocols.
Conclusions
The present review highlights the growing interest in PEMFs as a regenerative strategy for muscular and tendon lesions. Their non-invasive nature and favorable safety profile make PEMFs a promising adjunctive therapy in regenerative medicine.
Despite encouraging preclinical and early clinical findings, the evidence remains limited by methodological heterogeneity, small sample sizes, and inconsistent treatment protocols. Further high-quality translational and clinical studies are needed to standardize stimulation parameters, clarify optimal indications, and determine long-term clinical efficacy. Moreover, future research must differentiate among tendon types to better define the specific clinical contexts in which PEMF therapy may be most effective.
An emerging area of interest is the combination of PEMFs with regenerative cellular therapies, such as mesenchymal stem cells, to enhance cell survival, differentiation, and tissue repair. In parallel, recent research suggests that the early anabolic response to PEMF exposure is associated with the upregulation of early differentiation genes like c-fos49, indicating that PEMFs may act as upstream modulators directing progenitor cells toward osteogenic, chondrogenic, or tenogenic pathways depending on the local environment. Recent studies60-62 on mechanosensitive ion channels, particularly the PIEZO-type components (PIEZO)-1 and -2, which were awarded the 2021 Nobel Prize in Physiology or Medicine, offer further insights. Matsushima et al63 identified PIEZO-1 as a key sensor of mechanical stimuli in tenocytes, suggesting that PEMFs may exert some of their effects via activation of these channels, transducing mechanical cues into biological signals. Elucidating these pathways represents a critical frontier in PEMF research and may enable the development of more effective biophysical therapies.
Overall, PEMFs represent a biologically plausible and promising tool in musculoskeletal regenerative medicine, although further mechanistic and clinical research is required to fully define their therapeutic role.
Informed Consent:
Not applicable.
Ethics Approval:
Ethics approval was not required due to the nature of the study.
Conflict of Interest:
The authors declare no conflict of interest.
Authors’ Contributions:
Marmotti A. and Coco M. conceived the review and supervised the overall project. De Girolamo L., Di Matteo B., Vadalà G. and Mangiavini L. contributed to the design and coordination of the work and provided critical intellectual input. De Luca P., De Giorgi S., Carnevale A., Veronesi F., Berton A., Menon A., Ragni E., Anzillotti G., Giorgino R., Nannini A., Cucchi D., Rossi N., and Cavallo C. performed the literature search, organized the evidence, and drafted sections of the manuscript. Marmotti A., De Luca P., Coco M. and Setti S. critically revised the manuscript. All authors contributed to the writing process, approved the final version of the manuscript, and agreed to be accountable for its content.
ORCID ID:
A. Marmotti: 0000-0002-1683-6094
M. Coco: 0009-0002-8095-9862
P. De Luca: 0000-0001-9810-8818
S. De Giorgi: 0000-0002-0635-4964
A. Carnevale: 0000-0003-4543-1149
B. Di Matteo: 0000-0002-9807-0271
F. Veronesi: 0000-0002-6750-9376
A. Berton: 0000-0001-9767-7824
L. Mangiavini: 0000-0003-1892-1249
A. Menon: 0000-0003-2786-8099
L. de Girolamo: 0000-0002-9979-3092
E. Ragni: 0000-0003-0272-7417
G. Anzillotti: 0000-0001-9327-5350
R. Giorgino: 0000-0002-1067-7424
A. Nannini: 0000-0001-6742-2273
D. Cucchi: 0000-0001-6284-7977
N. Rossi: 0000-0003-4895-4789
C. Cavallo: 0000-0002-2913-856X
G. Vadalà: 0000-0001-7142-1660
S. Setti: 0000-0001-8990-5452
Funding:
None.
AI Disclosure:
AI tools were used during the preparation of this manuscript to assist with language refinement and editing. All scientific content, interpretation of the literature, critical analysis, and final approval of the manuscript were performed by the authors, who take full responsibility for the accuracy and integrity of the work.
References
- Cadossi R, Massari L, Racine-Avila J, Aaron RK. Pulsed Electromagnetic Field Stimulation of Bone Healing and Joint Preservation: Cellular Mechanisms of Skeletal Response. J Am Acad Orthop Surg Glob Res Rev 2020; 4: e1900155.
- Safavi AS, Sendera A, Haghighipour N, Banas-Zabczyk A. The Role of Low-Frequency Electromagnetic Fields on Mesenchymal Stem Cells Differentiation: A Systematic Review. Tissue Eng Regen Med 2022; 19: 1147-1160.
- Peng L, Fu C, Xiong F, Zhang Q, Liang Z, Chen L, He C, Wei Q. Effectiveness of Pulsed Electromagnetic Fields on Bone Healing: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Bioelectromagnetics2020; 41: 323-337.
- Gobbi A, Lad D, Petrera M, Karnatzikos G. Symptomatic Early Osteoarthritis of the Knee Treated With Pulsed Electromagnetic Fields: Two-Year Follow-Up. Cartilage 2014; 5: 78-85.
- Varani K, Vincenzi F, Pasquini S, Blo I, Salati S, Cadossi M, De Mattei M. Pulsed Electromagnetic Field Stimulation in Osteogenesis and Chondrogenesis: Signaling Pathways and Therapeutic Implications. Int J Mol Sci2021; 22: 809.
- Brighton CT, Wang W, Seldes R, Zhang G, Pollack SR. Signal Transduction in Electrically Stimulated Bone Cells. J Bone Joint Surg Am 2001; 83: 1514-1523.
- Mansourian M, Shanei A. Evaluation of Pulsed Electromagnetic Field Effects: A Systematic Review and Meta-Analysis on Highlights of Two Decades of Research In Vitro Studies. Biomed Res Int 2021; 2021: 6647497.
- Maziarz A, Kocan B, Bester M, Budzik S, Cholewa M, Ochiya T, Banas A. How Electromagnetic Fields Can Influence Adult Stem Cells: Positive and Negative Impacts. Stem Cell Res Ther 2016; 7: 54.
- Moretti L, Bizzoca D, Giancaspro GA, Cassano G.D, Moretti F, Setti S, Moretti B. Biophysical Stimulation in Athletes’ Joint Degeneration: A Narrative Review. Medicina (Kaunas) 2021; 57: 1206.
- Sui SX, Williams LJ, Holloway-Kew KL, Hyde NK, Pasco JA. Skeletal Muscle Health and Cognitive Function: A Narrative Review. Int J Mol Sci 2020; 22: 255.
- Frontera WR, Ochala J. Skeletal Muscle: A Brief Review of Structure and Function. Calcif Tissue Int 2015; 96: 183-195.
- Dumont NA, Bentzinger CF, Sincennes MC, Rudnicki MA. Satellite Cells and Skeletal Muscle Regeneration. Compr Physiol 2015; 5: 1027-1059.
- Yin H, Price F, Rudnicki MA. Satellite Cells and the Muscle Stem Cell Niche. Physiol Rev 2013; 93: 23-67.
- Sicari BM, Dearth CL, Badylak SF. Tissue Engineering and Regenerative Medicine Approaches to Enhance the Functional Response to Skeletal Muscle Injury. Anat Rec (Hoboken) 2014; 297: 51-64.
- Gandolfi S, Pileyre B, Drouot L, Dubus I, Auquit-Auckbur I, Martinet J. Stromal Vascular Fraction in the Treatment of Myositis. Cell Death Discov 2023; 9: 346.
- Di Rocco G, Iachininoto MG, Tritarelli A, Straino S, Zacheo A, Germani A, Crea F, Capogrossi MC. Myogenic Potential of Adipose-Tissue-Derived Cells. J Cell Sci 2006; 119: 2945-2952.
- Pinheiro CH, de Queiroz JC, Guimarães-Ferreira L, Vitzel KF, Nachbar RT, de Sousa LG, de Souza AL Jr, Nunes MT, Curi R. Local injections of adipose-derived mesenchymal stem cells modulate inflammation and increase angiogenesis ameliorating the dystrophic phenotype in dystrophin-deficient skeletal muscle. Stem Cell Rev Rep 2012; 8: 363-374.
- Kang Y, Park C, Kim D, Seong CM, Kwon K, Choi C. Unsorted Human Adipose Tissue-Derived Stem Cells Promote Angiogenesis and Myogenesis in Murine Ischemic Hindlimb Model. Microvasc Res 2010; 80: 310-316.
- Di Matteo B, Anzillotti G, Gallese A, Vitale U, Gaggia GMMC, Ronzoni FL, Marcacci M, Kon E. Placenta-Derived Products Demonstrate Good Safety Profile and Overall Satisfactory Outcomes for Treating Knee Osteoarthritis: A Systematic Review of Clinical Evidence. Arthroscopy 2023; 39: 1892-1904.
- Di Rocco G, Iachininoto MG, Tritarelli A, Straino S, Zacheo A, Germani A, Crea F, Capogrossi MC. Myogenic Potential of Adipose-Tissue-Derived Cells. J Cell Sci 2006; 119: 2945-2952.
- Pinheiro CH, de Queiroz JC, Guimarães-Ferreira L, Vitzel KF, Nachbar RT, de Sousa LG, de Souza AL Jr, Nunes MT, Curi R. Local injections of adipose-derived mesenchymal stem cells modulate inflammation and increase angiogenesis ameliorating the dystrophic phenotype in dystrophin-deficient skeletal muscle. Stem Cell Rev Rep 2012; 8: 363-374.
- Kang Y, Park C, Kim D, Seong CM, Kwon K, Choi C. Unsorted Human Adipose Tissue-Derived Stem Cells Promote Angiogenesis and Myogenesis in Murine Ischemic Hindlimb Model. Microvasc Res 2010; 80: 310-316.
- Terrie L, Burattini M, Van Vlierberghe S, Fassina L, Thorrez L. Enhancing Myoblast Fusion and Myotube Diameter in Human 3D Skeletal Muscle Constructs by Electromagnetic Stimulation. Front Bioeng Biotechnol2022; 10: 892287.
- Maiullari S, Cicirelli A, Picerno A, Giannuzzi F, Gesualdo L, Notarnicola A, Sallustio F, Moretti B. Pulsed Electromagnetic Fields Induce Skeletal Muscle Cell Repair by Sustaining the Expression of Proteins Involved in the Response to Cellular Damage and Oxidative Stress. Int J Mol Sci 2023; 24: 16631.
- Yang C, Xu L, Liao F, Liao C, Zhao Y, Chen Y, Yu Q, Peng B, Liu H. Pulsed Electromagnetic Fields Regulate Metabolic Reprogramming and Mitochondrial Fission in Endothelial Cells for Angiogenesis. Sci Rep 2024; 14: 19027.
- Ong MT, Man GC, Lau LC, He X, Qiu J, Wang Q, Chow MC, Choi BC, Yu M, Yung PS. Effect of pulsed electromagnetic field as an intervention for patients with quadriceps weakness after anterior cruciate ligament reconstruction: a double-blinded, randomized-controlled trial. Trials 2022; 23: 771.
- Jeon HS, Kang SY, Park JH, Lee HS. Effects of Pulsed Electromagnetic Field Therapy on Delayed-Onset Muscle Soreness in Biceps Brachii. Phys Ther Sport 2015; 16: 34-39.
- Trofè A, Piras A, Muehsam D, Meoni A, Campa F, Toselli S, Raffi M. Effect of Pulsed Electromagnetic Fields (PEMFs) on Muscular Activation during Cycling: A Single-Blind Controlled Pilot Study. Healthcare (Basel) 2023; 11: 922.
- Watkins JP, Auer JA, Morgan SJ, Gay S. Healing of Surgically Created Defects in the Equine Superficial Digital Flexor Tendon: Effects of Pulsing Electromagnetic Field Therapy on Collagen-Type Transformation and Tissue Morphologic Reorganization. Am J Vet Res 1985; 46: 2097-2103.
- Lee EW, Maffulli N, Li CK, Chan KM. Pulsed Magnetic and Electromagnetic Fields in Experimental Achilles Tendonitis in the Rat: A Prospective Randomized Study. Arch Phys Med Rehabil 1997; 78: 399-404.
- Strauch B, Patel MK, Rosen DJ, Mahadevia S, Brindzei N, Pilla AA. Pulsed Magnetic Field Therapy Increases Tensile Strength in a Rat Achilles’ Tendon Repair Model. J Hand Surg Am 2006; 31: 1131-1135.
- Tucker JJ, Cirone JM, Morris TR, Nuss CA, Huegel J, Waldorff EI, Zhang N, Ryaby JT, Soslowsky LJ. Pulsed Electromagnetic Field Therapy Improves Tendon-to-Bone Healing in a Rat Rotator Cuff Repair Model. J Orthop Res 2017; 35: 902-909.
- Huegel J, Choi DS, Nuss CA, Minnig MCC, Tucker JJ, Kuntz AF, Waldorff EI, Zhang N, Ryaby JT, Soslowsky LJ. Effects of pulsed electromagnetic field therapy at different frequencies and durations on rotator cuff tendon-to-bone healing in a rat model. J Shoulder Elbow Surg 2018; 27: 553-560.
- Dolkart O, Kazum E, Rosenthal Y, Sher O, Morag G, Yakobson E, Chechik O, Maman E. Effects of Focused Continuous Pulsed Electromagnetic Field Therapy on Early Tendon-to-Bone Healing. Bone Joint Res 2021; 10: 298-306.
- Huegel J, Chan PYW, Weiss SN, Nuss CA, Raja H, Waldorff EI, Zhang N, Ryaby JT, Soslowsky LJ, Kuntz AF. Pulsed Electromagnetic Field Therapy Alters Early Healing in a Rat Model of Rotator Cuff Injury and Repair: Potential Mechanisms. J Orthop Res 2022; 40: 1593-1603.
- Huegel J, Boorman-Padgett JF, Nuss CA, Raja HA, Chan PY, Kuntz AF, Waldorff EI, Zhang N, Ryaby JT, Soslowsky LJ. Effects of Pulsed Electromagnetic Field Therapy on Rat Achilles Tendon Healing. J Orthop Res 2020; 38: 70-81.
- Perucca Orfei C, Lovati AB, Lugano G, Viganò M, Bottagisio M, D’Arrigo D, Sansone V, Setti S, de Girolamo L. Pulsed electromagnetic fields improve the healing process of Achilles tendinopathy: a pilot study in a rat model. Bone Joint Res 2020; 9: 613-622.
- Uzun C, Erdal N, Gürgül S, Kalaycı D, Yılmaz ŞN, Özdemir AA, Yetkin D, Yılmaz C. Comparison of the Effects of Pulsed Electromagnetic Field and Extracorporeal Shockwave Therapy in a Rabbit Model of Experimentally Induced Achilles Tendon Injury. Bioelectromagnetics 2021; 42: 128-145.
- Pieber K, Schuhfried O, Fialka-Moser V. [Pulsed electromagnetic fields (PEMF)–results in evidence based medicine]. Wien Med Wochenschr 2007; 157: 34-36.
- Rosso F, Bonasia DE, Marmotti A, Cottino U, Rossi R. Mechanical Stimulation (Pulsed Electromagnetic Fields “PEMF” and Extracorporeal Shock Wave Therapy “ESWT”) and Tendon Regeneration: A Possible Alternative. Front Aging Neurosci 2015; 7: 211.
- Colombini A, Perucca Orfei C, Vincenzi F, De Luca P, Ragni E, Viganò M, Setti S, Varani K, de Girolamo L. A2A adenosine receptors are involved in the reparative response of tendon cells to pulsed electromagnetic fields. PLoS One 2020; 15: e0239807.
- de Girolamo L, Stanco D, Galliera E, Viganò M, Colombini A, Setti S, Vianello E, Corsi Romanelli MM, Sansone V. Low frequency pulsed electromagnetic field affects proliferation, tissue-specific gene expression, and cytokines release of human tendon cells. Cell Biochem Biophys 2013; 66: 697-708.
- de Girolamo L, Viganò M, Galliera E, Stanco D, Setti S, Marazzi MG, Thiebat G, Corsi Romanelli MM, Sansone V. In vitro functional response of human tendon cells to different dosages of low-frequency pulsed electromagnetic field. Knee Surg Sports Traumatol Arthrosc 2015; 23: 3443-3453.
- Vinhas A, Almeida AF, Rodrigues MT, Gomes ME. Prospects of Magnetically Based Approaches Addressing Inflammation in Tendon Tissues. Adv Drug Deliv Rev 2023; 196: 114815.
- Vinhas A, Gonçalves AI, Rodrigues MT, Gomes ME. Human Tendon-Derived Cell Sheets Created by Magnetic Force-Based Tissue Engineering Hold Tenogenic and Immunomodulatory Potential. Acta Biomater 2021; 131: 236-247.
- Vinhas A, Rodrigues MT, Gonçalves AI, Reis RL, Gomes ME. Pulsed Electromagnetic Field Modulates Tendon Cells Response in IL-1β-Conditioned Environment. J Orthop Res 2020; 38: 160-172.
- Gehwolf R, Schwemberger B, Jessen M, Korntner S, Wagner A, Lehner C, Weissenbacher N, Tempfer H, Traweger A. Global Responses of Il-1β-Primed 3D Tendon Constructs to Treatment with Pulsed Electromagnetic Fields. Cells 2019; 8: 399.
- Marmotti A, Mattia S, Mangiavini L, Bellato E, Ragni E, de Girolamo L, Peretti GM, Blonna D, Bonasia D, Setti S, Castoldi F. Hamstring grafts are tenogenic constructs for ACL reconstruction and Pulsed Electromagnetic Fields improve tendon specific markers expression. An in-vitro study. J Biol Regul Homeost Agents 2020; 34: 363-376.
- Marmotti A, Coco M, Orso F, Mangiavini L, de Girolamo L, Bellato E, Viganò M, Ragni E, Setti S, Taverna D, Castoldi F. The promising regenerative potential of pulsed electromagnetic fields toward tendon differentiation: a hamstring tendon explant culture study. Bone Joint Res 2026; 15: 167-178.
- Marmotti A, Peretti GM, Mattia S, Mangiavini L, de Girolamo L, Viganò M, Setti S, Bonasia DE, Blonna D, Bellato E, Ferrero G, Castoldi F. Pulsed Electromagnetic Fields Improve Tenogenic Commitment of Umbilical Cord-Derived Mesenchymal Stem Cells: A Potential Strategy for Tendon Repair-An In Vitro Study. Stem Cells Int 2018; 2018: 9048237.
- Viganò M, Sansone V, d’Agostino MC, Romeo P, Perucca Orfei C, de Girolamo L. Mesenchymal Stem Cells as Therapeutic Target of Biophysical Stimulation for the Treatment of Musculoskeletal Disorders. J Orthop Surg Res2016; 11: 163.
- Liu M, Lee C, Laron D, Zhang N, Waldorff EI, Ryaby JT, Feeley B, Liu X. Role of pulsed electromagnetic fields (PEMF) on tenocytes and myoblasts-potential application for treating rotator cuff tears. J Orthop Res 2017; 35: 956-964.
- Binder A, Parr G, Hazleman B, Fitton-Jackson S. Pulsed Electromagnetic Field Therapy of Persistent Rotator Cuff Tendinitis. A Double-Blind Controlled Assessment. Lancet 1984; 1: 695-698.
- Devereaux MD, Hazleman BL, Thomas PP. Chronic Lateral Humeral Epicondylitis–a Double-Blind Controlled Assessment of Pulsed Electromagnetic Field Therapy. Clin Exp Rheumatol 1985; 3: 333-336.
- Uzunca K, Birtane M, Taştekin N. Effectiveness of Pulsed Electromagnetic Field Therapy in Lateral Epicondylitis. Clin Rheumatol 2007; 26: 69-74.
- Osti L, Buono AD, Maffulli N. Pulsed Electromagnetic Fields after Rotator Cuff Repair: A Randomized, Controlled Study. Orthopedics 2015; 38: e223-e228.
- Klüter T, Krath A, Stukenberg M, Gollwitzer H, Harrasser N, Knobloch K, Maffulli N, Hausdorf J, Gerdesmeyer L. Electromagnetic transduction therapy and shockwave therapy in 86 patients with rotator cuff tendinopathy: A prospective randomized controlled trial. Electromagn Biol Med 2018; 37: 175-183.
- Özdemir M, Yaşar MF, Yakşi E. Effect of Pulsed Electromagnetic Field Therapy in Patients with Supraspinatus Tendon Tear. Rev Assoc Med Bras (1992) 2021; 67: 282-286.
- Ko VMC, He X, Fu SC, Yung PSH, Ling SKK. Clinical Effectiveness of Pulsed Electromagnetic Field Therapy as an Adjunct Treatment to Eccentric Exercise for Achilles Tendinopathy: A Randomized Controlled Trial. Trials2023; 24: 394.
- Passini FS, Jaeger PK, Saab AS, Hanlon S, Chittim NA, Arlt MJ, Ferrari KD, Haenni D, Caprara S, Bollhalder M, Niederöst B, Horvath AN, Götschi T, Ma S, Passini-Tall B, Fucentese SF, Blache U, Silván U, Weber B, Silbernagel KG, Snedeker JG. Shear-stress sensing by PIEZO1 regulates tendon stiffness in rodents and influences jumping performance in humans. Nat Biomed Eng 2021; 5: 1457-1471.
- Nakamichi R, Ma S, Nonoyama T, Chiba T, Kurimoto R, Ohzono H, Olmer M, Shukunami C, Fuku N, Wang G, Morrison E, Pitsiladis YP, Ozaki T, D’Lima D, Lotz M, Patapoutian A, Asahara H. The mechanosensitive ion channel PIEZO1 is expressed in tendons and regulates physical performance. Sci Transl Med 2022; 14: 5557.
- Götschi T, Held V, Klucker G, Niederöst B, Aagaard P, Spörri J, Passini FS, Snedeker JG. PIEZO1 gain-of-function gene variant is associated with elevated tendon stiffness in humans. J Appl Physiol (1985) 2023; 135: 165-173.
- Matsushima T, Hiroshi A. Molecular Mechanisms of Mechanosensing and Plasticity of Tendons and Ligaments. J Biochem 2024; 176: 263-269.
To cite this article
Pulsed electromagnetic fields in muscle and tendon injuries: a narrative review of preclinical and clinical evidence
JOINTS 2026;
4: e2116
DOI: 10.26355/joints_202606_2116
Publication History
Submission date: 16 Sep 2025
Revised on: 18 Dec 2025
Accepted on: 04 Jun 2026
Published online: 12 Jun 2026